Obstructive vs Restrictive Lung Disease: Differences, Similarities, & Diagnosis
.avif)

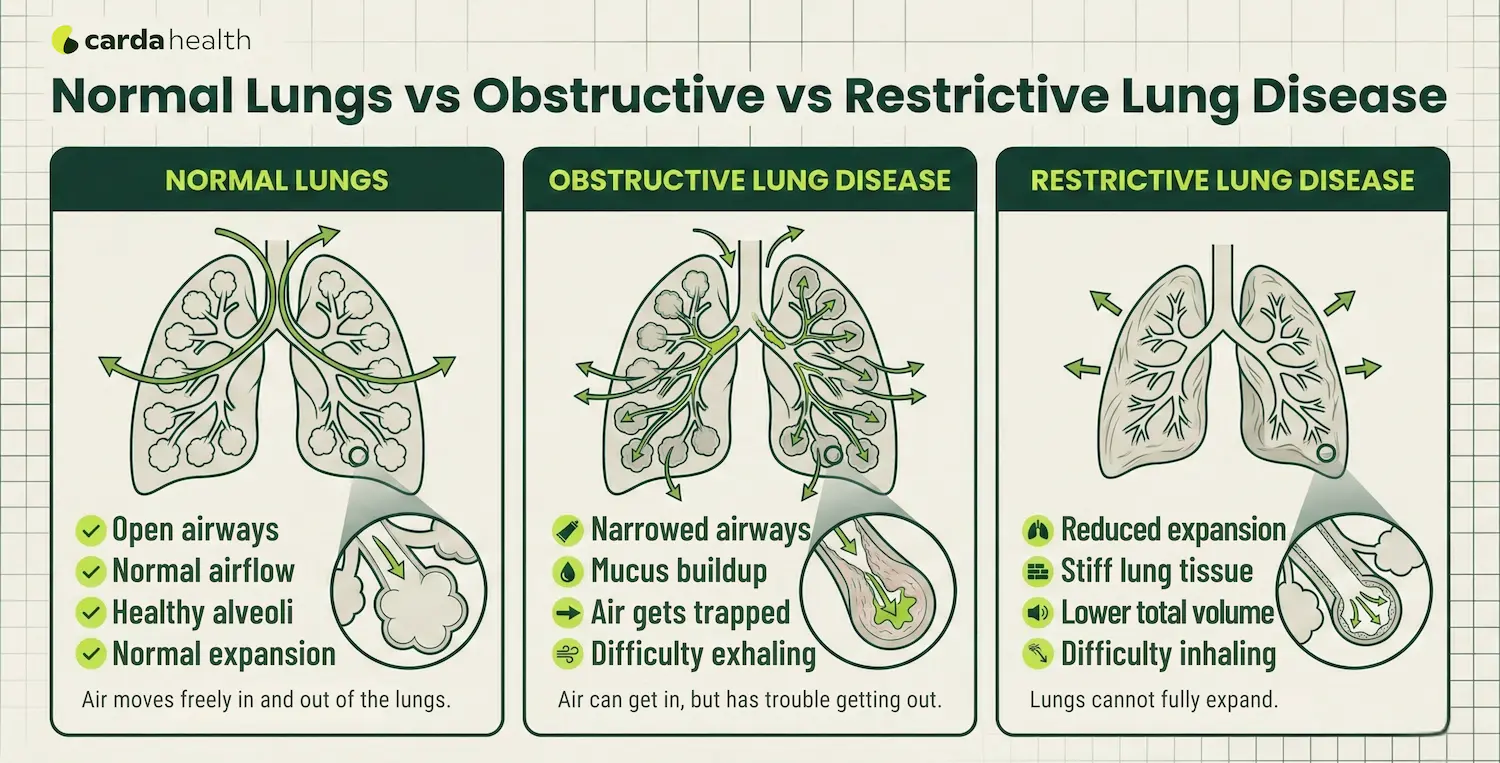
If you've been told you have an "obstructive" or "restrictive" lung problem, the terms can sound confusing. Both affect breathing, but they do so in very different ways. In simplest terms:
Obstructive lung disease makes it hard to get air out of your lungs because the airways are narrowed or blocked.
Restrictive lung disease makes it hard to fully expand your lungs, so you can't take in as much air as normal.
Understanding this difference matters. It affects how doctors interpret breathing tests, what treatments are prescribed, and what to expect long term.
What Is Obstructive Lung Disease?
Obstructive lung disease is a group of conditions where airflow is limited because the airways are narrowed, inflamed, or blocked. The main problem is getting air out. When the airways collapse or become clogged with mucus, air gets trapped inside the lungs. This leads to a feeling of incomplete exhalation and shortness of breath.
Common Examples of Obstructive Lung Disease
- COPD (Chronic Obstructive Pulmonary Disease)
- Chronic bronchitis
- Emphysema
- Asthma
- Bronchiectasis
Typical Symptoms
People with obstructive lung disease often experience shortness of breath, especially during physical activity. Wheezing is common, along with a chronic cough that may produce mucus. Because the airways are narrowed, exhaling can take longer than normal, leading to a sensation of trapped air in the chest. Over time, these symptoms may gradually worsen, particularly in conditions like COPD.
What Do Lung Function Tests Show?
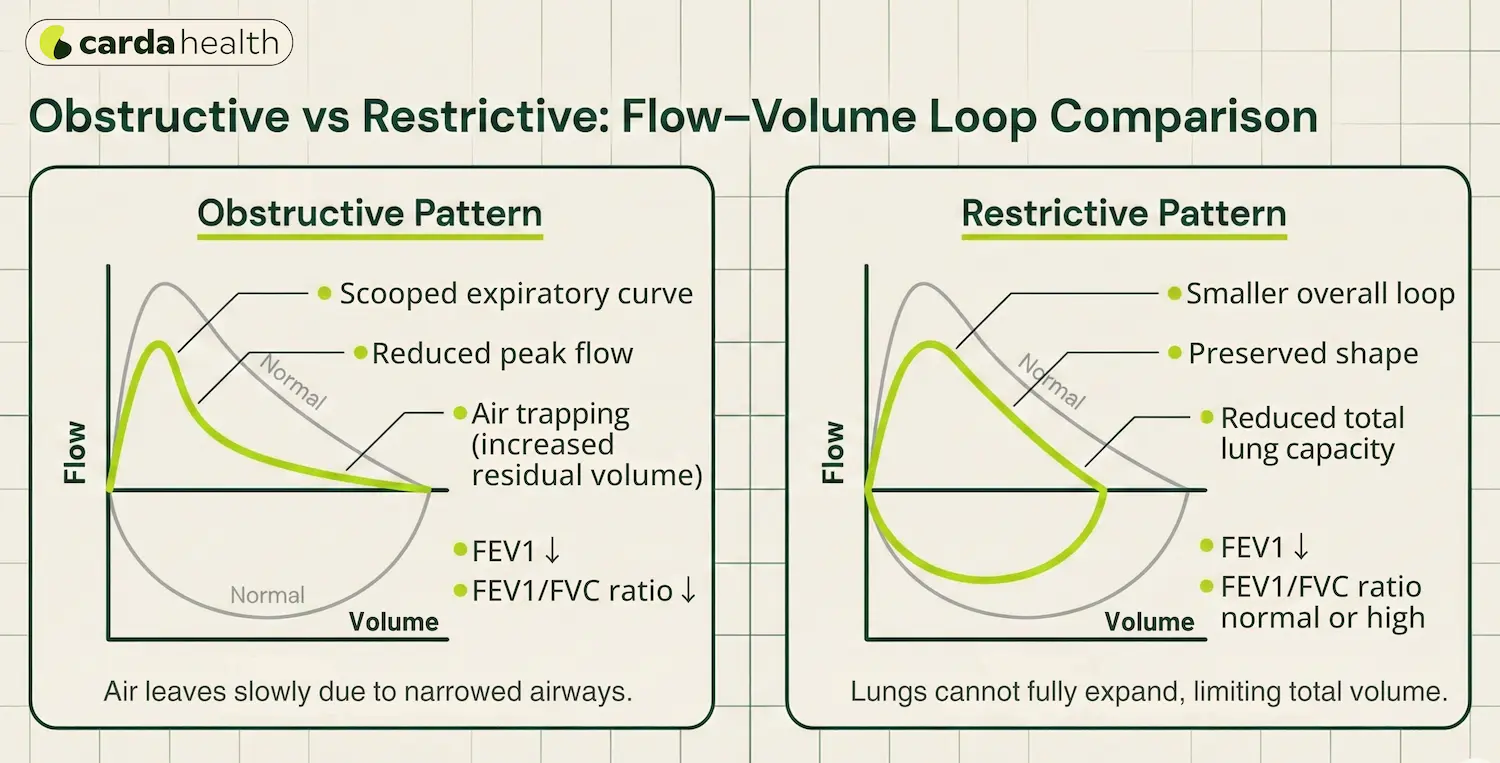
On spirometry, obstructive disease typically shows Low FEV₁ (forced expiratory volume in 1 second) & Low FEV₁/FVC ratio (usually < 0.70 after bronchodilator in COPD) which results in normal or increased total lung capacity (due to air trapping).
In simple terms: the lungs may be full of air, but that air can't escape efficiently.
What Is Restrictive Lung Disease?
Restrictive lung disease is a group of conditions where the lungs cannot fully expand, so less air enters with each breath. Opposite to the obstructive lung disease, the problem here isn't blocked airways, it's reduced lung capacity. The lungs simply cannot hold as much air as they should. This makes each breath smaller and can cause breathlessness, especially during activity.
Common Examples of Restrictive Lung Disease
- Pulmonary fibrosis
- Interstitial lung disease (ILD)
- Sarcoidosis
- Chest wall disorders (severe scoliosis)
- Neuromuscular diseases (e.g., ALS, muscular dystrophy)
- Obesity-related restriction
Typical Symptoms
Restrictive lung disease usually causes progressive shortness of breath, meaning it slowly becomes more noticeable over time. A dry, persistent cough is common, especially in conditions like pulmonary fibrosis. Breathing may feel shallow or rapid because the lungs cannot fully expand. Many people also notice early fatigue during activity, as reduced lung capacity limits oxygen delivery to the body.
What Do Lung Function Tests Show?
On lung function testing, doctors usually find reduced FVC (forced vital capacity), normal or high FEV₁/FVC ratio, which means low total lung capacity (TLC) on full pulmonary function testing.
In simple terms: airflow may be normal, but the lungs are smaller or stiffer than they should be.
{{get-started}}
How Doctors Diagnose Obstructive vs Restrictive Lung Disease
Doctors don't rely on symptoms alone. Shortness of breath can look similar in both conditions. The real difference shows up on pulmonary function tests (PFTs).
1. Spirometry (First Step)
Spirometry measures how much air you can blow out and how fast.
Key numbers doctors look at:
FEV₁: How much air you force out in 1 second
FVC: Total air you can blow out
FEV₁/FVC ratio: The most important comparison
Pattern:
- Low FEV₁/FVC → Obstructive pattern
- Normal or high FEV₁/FVC + low FVC → Possible restrictive pattern
If spirometry suggests restriction, doctors usually order more testing.
2. Full Pulmonary Function Testing
This includes lung volume testing to measure:
a) Total Lung Capacity (TLC)
b) Residual Volume (RV)
If TLC is low, that confirms restrictive lung disease. If TLC is normal or high with air trapping, that supports obstructive disease.
3. Diffusion Capacity (DLCO)
The diffusion capacity test (DLCO) measures how efficiently oxygen moves from the lungs into the bloodstream. This test helps doctors understand whether the issue involves the air sacs or the lung tissue itself.
DLCO is often reduced in emphysema because the air sacs are damaged, and it is commonly reduced in interstitial lung disease due to scarring of the lung tissue. In asthma, DLCO may remain normal.
Also Read: COPD vs Asthma: Symptoms, Risks, and Key Differences
This information helps clinicians narrow down the underlying cause and determine whether the pattern is primarily obstructive, restrictive, or mixed.
4. Imaging (Chest X-ray or CT Scan)
Imaging can show:
- Hyperinflated lungs (commonly barrel chest in COPD)
- Scarring or fibrosis (seen in restrictive diseases)
- Structural abnormalities
The diagnosis isn't just about labeling a condition, it determines what kind of treatment will actually help you breathe better.
Treatment: Why the Approach Is Different
Treatment depends entirely on whether the problem is airflow obstruction or lung restriction. The goals are different, and so are the medications and therapies.
Treating Obstructive Lung Disease
Because air is getting trapped in the lungs, treatment focuses on opening the airways and reducing inflammation.
Common strategies include:
- Bronchodilators (inhalers) to relax airway muscles
- Inhaled corticosteroids (ICS) in selected patients (especially asthma or frequent COPD flare-ups)
- Combination inhalers (LABA/LAMA or triple therapy in COPD)
- Pulmonary rehabilitation to improve breathing efficiency
- Smoking cessation (critical in COPD)
- Vaccines to reduce infection risk
- Oxygen therapy in advanced disease
In asthma, symptoms can often be well controlled. In COPD, treatment aims to slow progression and improve quality of life.
Treating Restrictive Lung Disease
Here, the lungs cannot fully expand. So treatment focuses on addressing the underlying cause and improving oxygen levels.
Depending on the condition, doctors may recommend:
- Anti-fibrotic medications (for idiopathic pulmonary fibrosis)
- Immunosuppressants or steroids (for inflammatory causes)
- Weight management (if obesity contributes)
- Chest wall or neuromuscular support therapies
- Pulmonary rehabilitation
- Oxygen therapy if oxygen levels are low
Also Read: How to Increase Oxygen Levels: Safe & Simple Home Steps
Unlike obstructive disease, inhalers are often less effective in purely restrictive conditions unless airway obstruction is also present.
The Overlap Treatment
Some patients show both obstructive and restrictive patterns on testing. In those cases, treatment plans are individualized, often combining inhalers, rehab, and oxygen support.
Obstructive vs Restrictive Lung Disease Comparison
Here's a clear comparison to help you quickly understand the difference:
Can Someone Have Both?
Yes. Some people have a mixed pattern, meaning they have elements of both obstruction and restriction.
For example a person with long-standing COPD who also develops pulmonary fibrosis, or severe obesity combined with asthma, or smoking-related COPD plus scarring from prior lung infections.
In these cases, pulmonary function testing becomes especially important to guide treatment decisions.
Also Read: How to Test Yourself For COPD: At-Home Assessment Steps
{{get-started}}
When to See a Doctor
If you experience persistent shortness of breath, chronic cough lasting more than 8 weeks, wheezing, reduced exercise tolerance, or unexplained fatigue, you should see your doctor immediately.
A doctor may recommend spirometry or full pulmonary function testing to determine whether the issue is obstructive, restrictive, or mixed. Early diagnosis matters. Many lung diseases are easier to manage before severe damage occurs.
Conclusion
Obstructive and restrictive lung diseases affect breathing in very different ways. One makes it hard to push air out. The other makes it hard to pull air in. Understanding the difference helps guide the right testing, the right treatment, and the right long-term plan.
If you're living with chronic breathing issues, getting accurate lung testing is the first step toward breathing easier, and protecting your long-term lung health.
FAQs
What is the main difference between obstructive and restrictive lung disease?
Obstructive lung disease makes it difficult to exhale air fully because the airways are narrowed or blocked. Restrictive lung disease makes it difficult to inhale fully because the lungs cannot expand properly. The difference is confirmed through spirometry testing.
How can you tell if a lung disease is obstructive or restrictive?
In obstructive disease, the FEV₁/FVC ratio is reduced. In restrictive disease, the FVC is reduced, but the FEV₁/FVC ratio is usually normal or high.
Is asthma obstructive or restrictive?
Asthma is an obstructive lung disease. It causes airway inflammation and narrowing, which makes it hard to breathe out. Unlike COPD, asthma is often partially or fully reversible with treatment.
Is COPD obstructive or restrictive?
COPD (chronic obstructive pulmonary disease) is an obstructive lung disease. It causes airflow limitation and air trapping, making exhalation difficult. It is generally progressive and not fully reversible.
Can someone have both obstructive and restrictive lung disease?
Yes. This is called a mixed pattern on pulmonary function testing. It can occur in people with conditions like COPD plus pulmonary fibrosis, or obesity combined with asthma.
References
https://www.webmd.com/lung/obstructive-and-restrictive-lung-disease
https://geekymedics.com/spirometry-interpretation
https://www.ncbi.nlm.nih.gov/books/NBK560880/
https://www.aafp.org/pubs/afp/issues/2014/0301/p359.html



