

Key Takeaways
A heart attack occurs when blood flow to the heart is blocked. A stroke occurs when blood flow to the brain is interrupted. Both are life-threatening emergencies with overlapping risk factors, but they produce different symptoms and require different treatments. Recognizing which one is happening, and acting immediately, can save a life.
What Is a Heart Attack?
A heart attack, medically known as a myocardial infarction, happens when one or more of the coronary arteries that supply blood to the heart muscle become blocked. The blockage is usually caused by a buildup of cholesterol-rich plaque inside the artery walls, a condition called atherosclerosis. When a plaque ruptures, a blood clot forms at the site and can completely stop blood flow. Without oxygen, heart muscle cells begin to die within minutes.
Cardiologists use the phrase "time is muscle" to emphasize the urgency: the longer the artery stays blocked, the more heart tissue is permanently damaged. Rapid treatment, ideally within 60 to 90 minutes, can restore blood flow and dramatically improve outcomes.
For a deeper look at what happens during and after a heart attack, see our guide on what happens after a heart attack.
Also read: widowmaker heart attack.
What Is a Stroke?
A stroke happens when the blood supply to part of the brain is suddenly cut off or when a blood vessel in the brain bursts. Without oxygen, brain cells begin to die rapidly. Neurologists use the parallel phrase "time is brain" — every minute of delayed treatment increases the risk of permanent brain damage.
There are three main types of stroke. Ischemic strokes account for roughly 87% of all strokes and are caused by a blood clot blocking an artery in the brain, a mechanism very similar to a heart attack. Hemorrhagic strokes occur when a blood vessel in the brain ruptures, causing bleeding into or around the brain tissue. Transient ischemic attacks (TIAs), often called mini-strokes, involve a temporary blockage that resolves on its own, usually within minutes to hours. TIAs rarely cause permanent damage, but they are a serious warning sign of a future stroke.
Also see our article on mini-stroke recovery.
Key Differences Stroke vs. Heart Attack
While stroke and heart attack share a common underlying problem — disrupted blood flow — they differ in almost every other respect. The table below summarizes the most important distinctions.
{{get-started}}
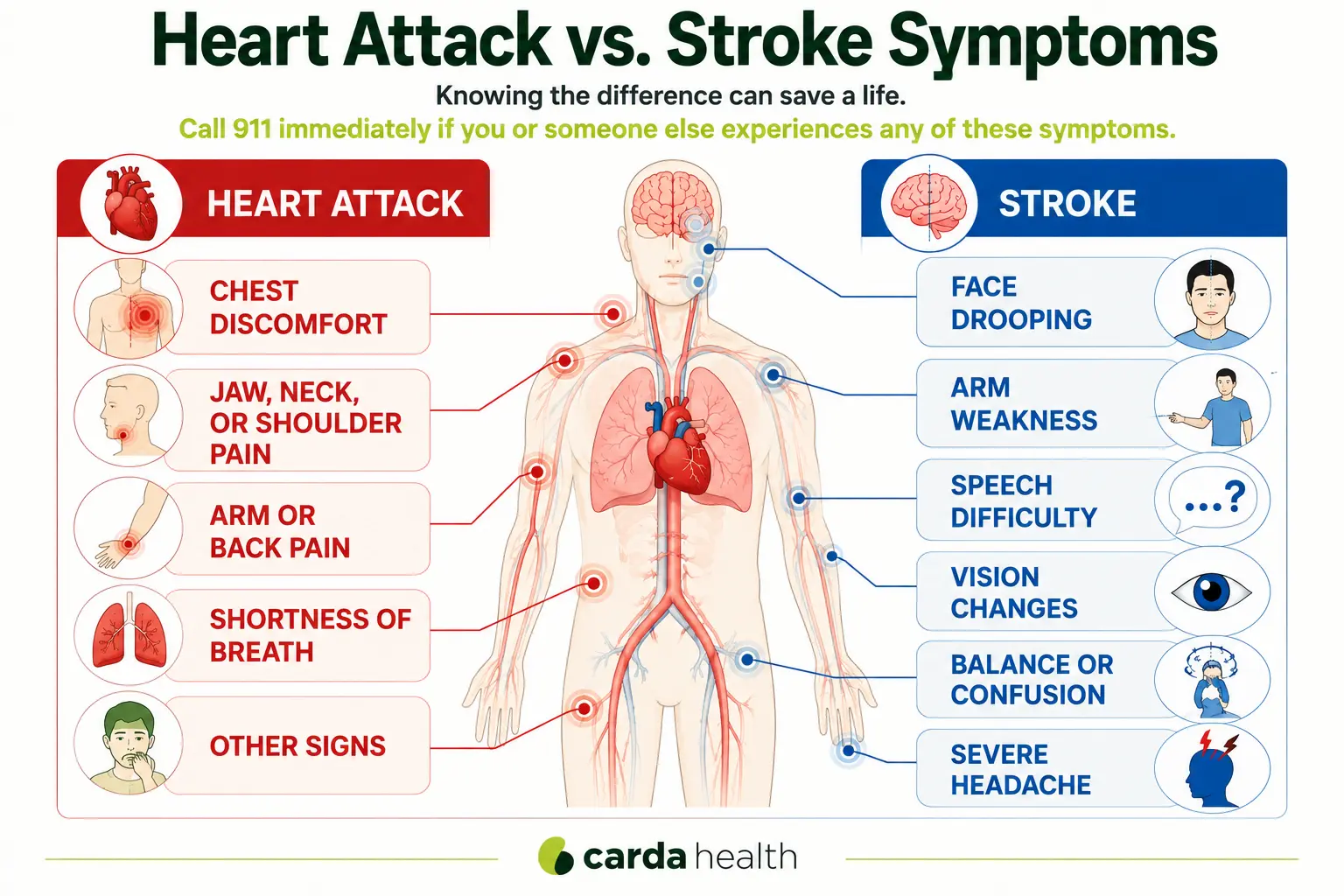
Stroke vs Heart Attack Symptoms
Heart attack symptoms tend to center on the chest and upper body. The most common sign is chest pain or pressure, often described as tightness, squeezing, or a heavy weight on the chest. This discomfort may radiate to the left arm, jaw, neck, shoulder, or back. Other warning signs include shortness of breath, a cold sweat, nausea, lightheadedness, and unusual fatigue. Symptoms may come on suddenly or build gradually over minutes to hours.
Stroke symptoms are neurological rather than cardiac. They typically appear suddenly and affect one side of the body. The American Heart Association recommends using the acronym FAST to spot a stroke: Face drooping (one side of the face is numb or drooping), Arm weakness (one arm drifts downward when both are raised), Speech difficulty (slurred or garbled speech), and Time to call 911. Additional stroke symptoms include sudden confusion, trouble seeing in one or both eyes, severe headache with no known cause, and sudden difficulty walking or maintaining balance.
A critical safety distinction: if you suspect a heart attack, chewing an aspirin (if not allergic) can help reduce blood clotting while waiting for emergency services. But if you suspect a stroke, do NOT give aspirin. Aspirin could worsen a hemorrhagic stroke by increasing bleeding in the brain. Only medical professionals, after imaging confirms the stroke type, can determine whether blood-thinning treatment is safe.
Symptoms in women deserve extra attention. For both conditions, women are more likely to experience atypical symptoms. Heart attack symptoms in women may include unusual fatigue, upper back discomfort, nausea, or jaw pain rather than classic chest pressure. Stroke symptoms in women may include sudden hiccups, general weakness, chest pain, or sudden nausea. These less obvious presentations can delay recognition and treatment.
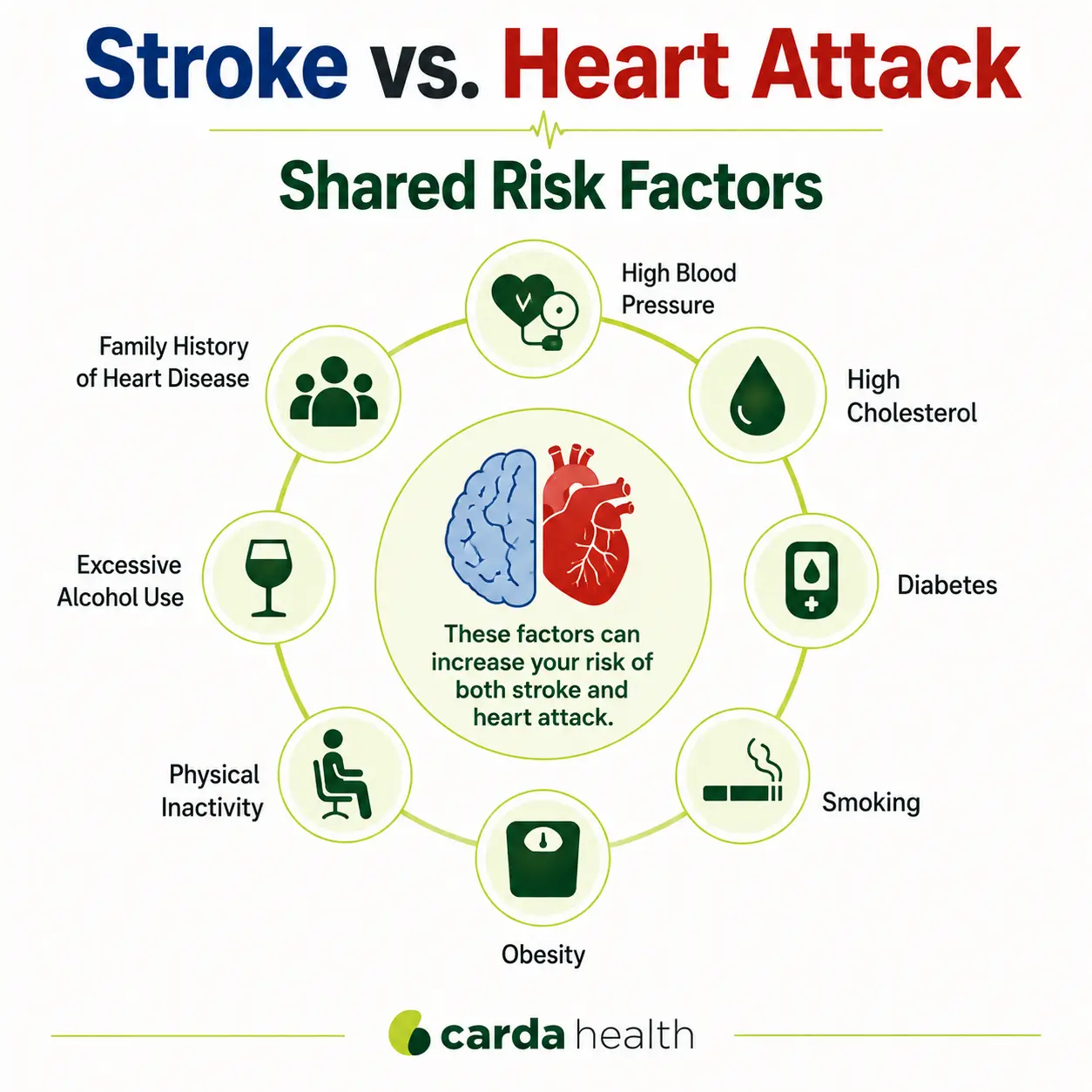
Shared Risk Factors
The most significant shared risk factors include high blood pressure (the single greatest contributor to both conditions), high LDL cholesterol, diabetes, smoking, obesity, physical inactivity, excessive alcohol use, and family history of cardiovascular disease.
Atrial fibrillation (AFib) is a particularly important risk factor for stroke that is directly linked to heart disease. AFib is an irregular heart rhythm that causes blood to pool in the heart's upper chambers, where clots can form. If a clot travels from the heart to the brain, it causes an ischemic stroke. According to Mayo Clinic, atrial fibrillation contributes to nearly 20% of all stroke cases. People with heart failure are two to three times more likely to have a stroke compared to those without it.
To understand more about how these conditions are interconnected, see our article on how hypertension, heart disease, and stroke are related.
Also read our guide on what is a heart flutter.
Treatment: How Each Emergency Is Handled
Both conditions demand immediate emergency care, but the specific treatments differ because the organs involved and the underlying mechanisms are not the same.
For a heart attack, the primary goal is to reopen the blocked coronary artery as quickly as possible. Emergency teams administer aspirin and blood thinners, and the patient is typically taken to the cardiac catheterization lab for percutaneous coronary intervention (PCI), a procedure in which a balloon-tipped catheter opens the artery and a stent is placed to keep it open. In cases of severe or multi-vessel blockage, coronary artery bypass graft (CABG) surgery may be needed. After the acute phase, patients are placed on a regimen of medications including statins, beta-blockers, ACE inhibitors, and antiplatelet drugs.
Also read: cardiac enzymes and heart attacks.
For an ischemic stroke, the first-line treatment is a clot-dissolving drug called tPA (tissue plasminogen activator), which must be administered within 4.5 hours of symptom onset for the best results. In some cases, a mechanical thrombectomy — a procedure that physically removes the clot using a catheter — is performed. For a hemorrhagic stroke, the approach is very different: surgeons may need to clip or coil the ruptured blood vessel, and blood pressure must be aggressively managed. Blood thinners are avoided because they would worsen the bleeding.
Recovery and Rehabilitation
Recovery after a heart attack typically involves a structured cardiac rehabilitation program — a medically supervised combination of exercise training, nutritional guidance, education, and psychosocial support. Most patients begin rehab within a few weeks of discharge and complete 36 sessions over approximately 12 weeks. The CDC reports that completing cardiac rehab reduces cardiovascular death risk by nearly 45% and hospital readmissions by about 30%.
Recovery after a stroke is more variable and depends heavily on which part of the brain was affected and how much tissue was damaged. If the stroke was caused by or occurred alongside heart disease, cardiac rehabilitation may also be recommended to address the underlying cardiovascular risk factors.
Recovery is not just about surviving the event — it's about building the habits, support systems, and medical foundation that protect you going forward.
Explore our guides on what is heart rehab, virtual cardiac rehab, and exercises after a heart attack.
How to Reduce Your Risk of Both
Because stroke and heart attack share so many risk factors, the prevention strategies are largely the same. Managing blood pressure is the single most impactful step you can take. Beyond that, keeping cholesterol and blood sugar in healthy ranges, quitting smoking, staying physically active (at least 150 minutes of moderate exercise per week), eating a heart-healthy diet, limiting alcohol, and maintaining regular check-ups with your healthcare provider all significantly reduce your risk.
If you have atrial fibrillation or a history of heart disease, working closely with your cardiologist to manage these conditions is especially important for stroke prevention. And if you've experienced a TIA (mini-stroke), treat it as an urgent warning sign — prompt evaluation and treatment can prevent a full stroke from occurring.
{{get-started}}
FAQs
What is the main difference between a stroke and a heart attack?
A heart attack affects the heart — it happens when blood flow to the heart muscle is blocked. A stroke affects the brain — it happens when blood flow to the brain is interrupted or a blood vessel in the brain ruptures. Both are emergencies that require immediate medical attention.
Can you have a stroke and a heart attack at the same time?
It is rare but possible. A heart attack can trigger an irregular heart rhythm or reduce blood flow enough to cause a stroke. The two events can also occur independently in someone with advanced cardiovascular disease affecting both the coronary and cerebral arteries.
Which is worse, a stroke or a heart attack?
Neither is inherently "worse" — both can be fatal or cause lasting disability. Outcomes depend on the severity of the event, how quickly treatment is received, and the patient's overall health.
Can a heart attack lead to a stroke?
Yes. According to research published by Harvard Health, heart attack survivors have an elevated risk of stroke, particularly in the year following the event. Heart damage can lead to clot formation, trigger atrial fibrillation, or reduce overall cardiac output — all of which increase stroke risk.
Should you give aspirin if someone is having a stroke?
No. Unlike a heart attack, where aspirin can help, giving aspirin during a stroke can be dangerous. If the stroke is hemorrhagic (caused by bleeding), aspirin can worsen the bleed. Only medical professionals can determine the stroke type through imaging and decide whether blood thinners are appropriate.
References
- American Heart Association. Heart Attack, Stroke and Cardiac Arrest Symptoms. heart.org.
- Cleveland Clinic. Stroke vs. Heart Attack: What's the Difference? health.clevelandclinic.org.
- Mayo Clinic. The Link Between Heart Disease and Stroke. newsnetwork.mayoclinic.org.
- Harvard Health Publishing. Stroke After a Heart Attack: What's the Risk? health.harvard.edu.
- Centers for Disease Control and Prevention. Cardiac Rehabilitation. cdc.gov.
- American Stroke Association. Types of Stroke. stroke.org.
- National Heart, Lung, and Blood Institute (NHLBI). Ischemic Stroke. nhlbi.nih.gov.
- Reitan C, et al. Excess Mortality and Loss of Life Expectancy After Myocardial Infarction. Circulation. 2024.


