

Key Takeaways
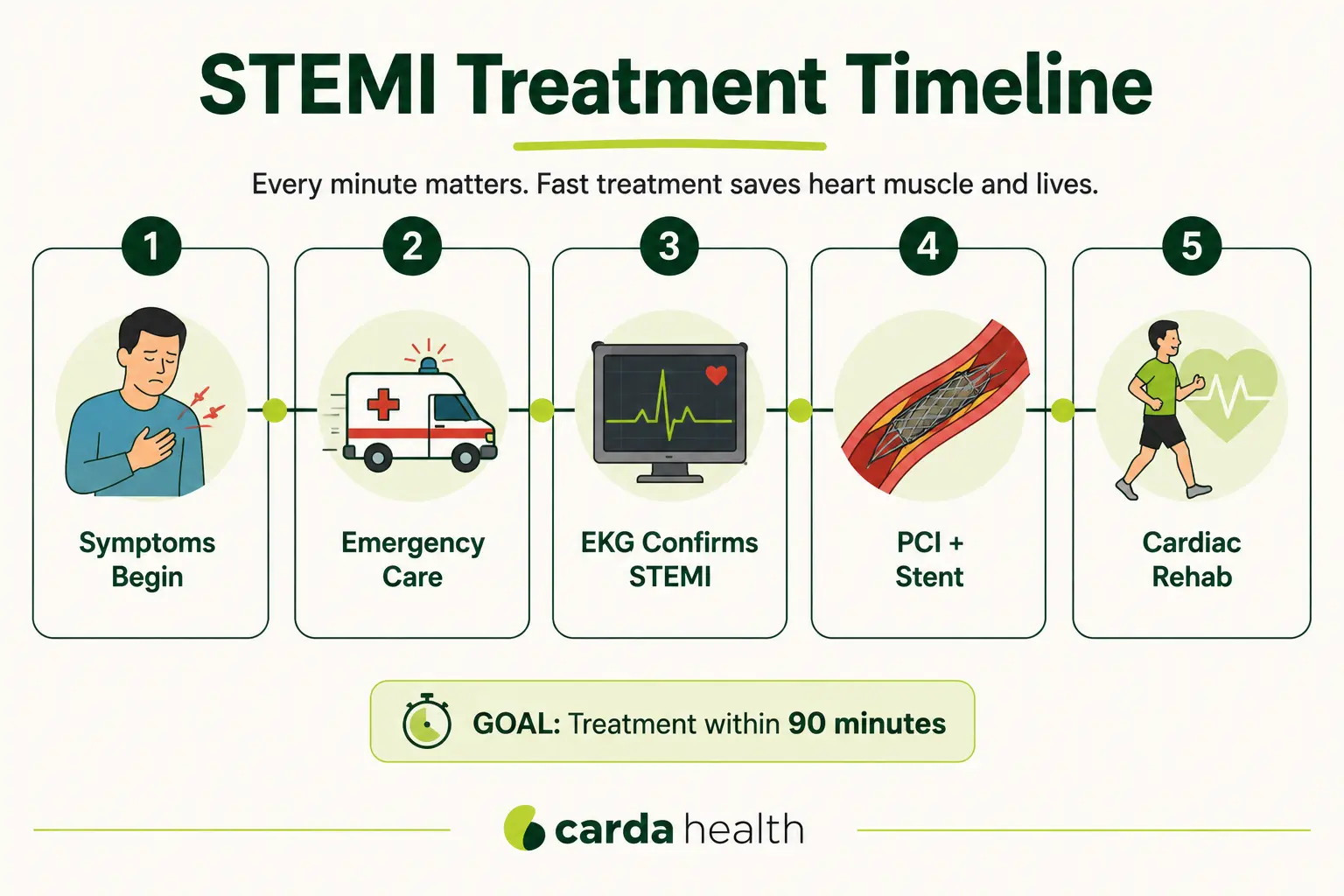
A STEMI (ST-elevation myocardial infarction) is a severe type of heart attack caused by a complete blockage of a coronary artery. It accounts for about 30% of all heart attacks and carries a higher risk of complications and death than other types. With rapid treatment, ideally within 90 minutes, in-hospital survival rates exceed 90%. Recovery includes medications, lifestyle changes, and cardiac rehabilitation.
What Is a STEMI Heart Attack?
A STEMI, short for ST-elevation myocardial infarction, is the most severe type of heart attack. It occurs when one of the coronary arteries that supply blood to the heart becomes completely blocked, cutting off blood flow entirely to a portion of the heart muscle. Without blood and oxygen, the affected heart muscle begins to die within minutes.
According to the National Library of Medicine, approximately 30% of all heart attacks are STEMIs. While less common than NSTEMIs (which involve a partial blockage), STEMIs carry a higher risk of serious complications and death because the artery is completely obstructed.
A STEMI falls under the umbrella of acute coronary syndrome (ACS), which also includes NSTEMI and unstable angina.
Also read our guide on angina vs. heart attack.
Characteristics of a STEMI
Both STEMI and NSTEMI are heart attacks that damage the heart muscle, but they differ in severity, diagnosis, and urgency of treatment.
Also Read: stable vs. unstable angina.
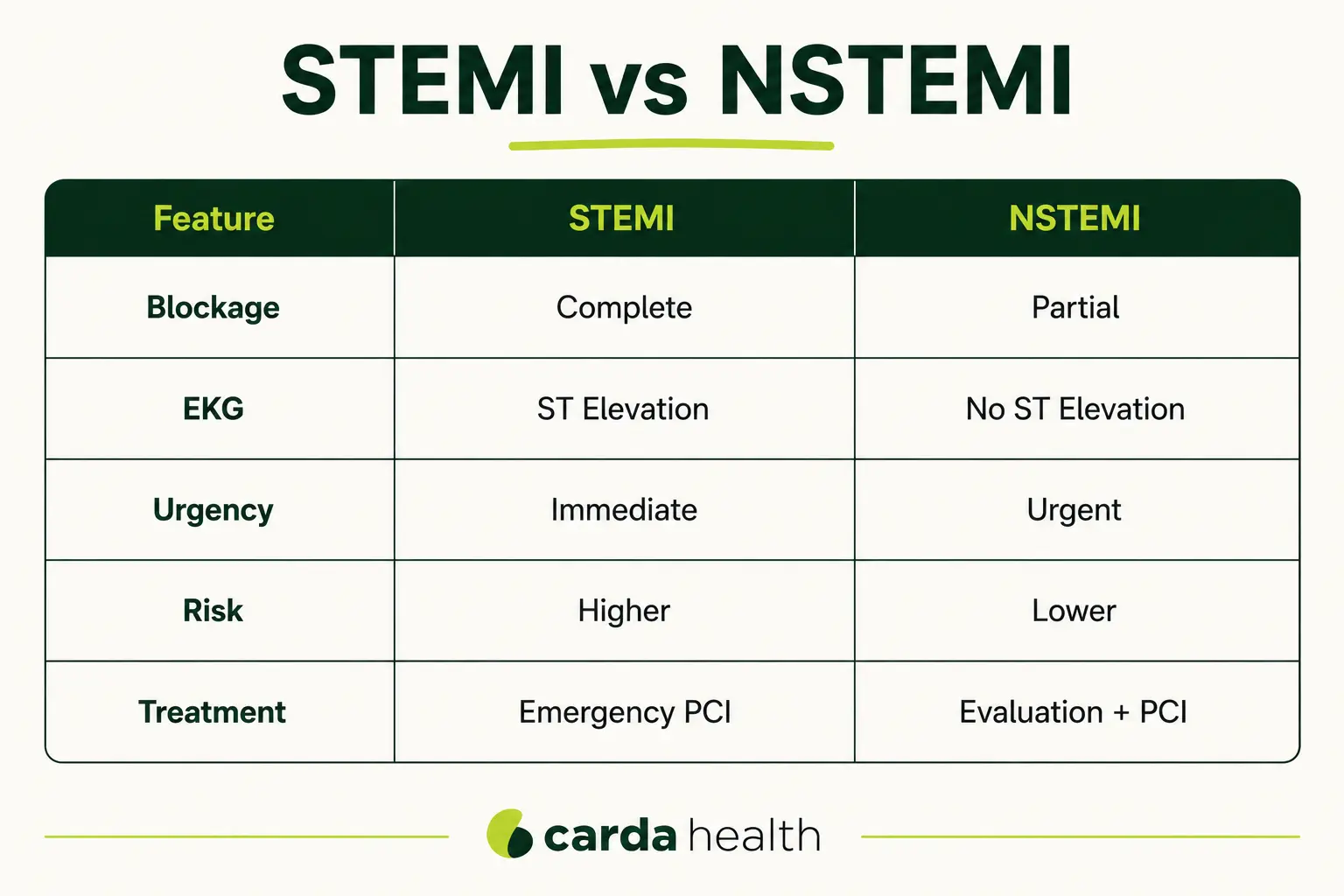
STEMI vs NSTEMI: What Is the Difference?
Both STEMI and NSTEMI are forms of acute myocardial infarction (heart attack), but they differ in how severely blood flow is affected and how urgently treatment is typically required.
A STEMI usually occurs when a coronary artery becomes completely blocked, cutting off blood flow entirely to part of the heart muscle. An NSTEMI, on the other hand, generally involves a partial blockage, meaning some blood flow is still reaching the heart.
Although STEMIs often require faster intervention because of complete vessel occlusion, both conditions are medical emergencies and can lead to serious complications if treatment is delayed.
Symptoms of a STEMI Heart Attack
You cannot tell from symptoms alone whether you are having a STEMI or another type of heart attack. The symptoms are the same across all heart attack types. Only medical testing, specifically an EKG and blood tests, can determine the type.
Common symptoms include chest pain or pressure (often described as tightness, squeezing, or heaviness), pain radiating to the arms, jaw, neck, shoulders, or back, shortness of breath, cold sweat, nausea or vomiting, lightheadedness or dizziness, and a sense of impending doom.
Symptoms in women may present differently. Women are more likely to experience atypical signs such as unusual fatigue, upper back discomfort, nausea, jaw pain, or shortness of breath without classic chest pressure.
{{get-started}}
Causes and Risk Factors
What Causes a STEMI
The vast majority of STEMIs are caused by atherosclerosis, the gradual buildup of cholesterol-rich plaque inside the coronary arteries. A STEMI occurs when one of these plaques becomes unstable, ruptures, and triggers the formation of a blood clot large enough to completely block the artery. This sequence, plaque rupture followed by thrombotic occlusion, happens rapidly, often within minutes, and is what makes a STEMI such an acute emergency.
In rare cases, a STEMI can be caused by a coronary artery spasm (a sudden, severe tightening of the artery wall) or spontaneous coronary artery dissection (SCAD), in which the artery wall tears without traditional risk factors being present.
Risk Factors
The risk factors for a STEMI are the same as for coronary artery disease in general: high blood pressure, high LDL cholesterol, diabetes, smoking (the strongest modifiable risk factor), obesity, physical inactivity, family history of heart disease, and advancing age.
Men are at increased risk after age 45, and women after age 50, though STEMIs can occur at any age.
What To Do If You Think You Are Having a STEMI
If you think you or someone nearby may be experiencing symptoms of a heart attack, treat it as a medical emergency. Fast treatment can significantly improve outcomes and reduce damage to the heart muscle.
Take these steps immediately:
- Call 911 or local emergency services right away
- Do not drive yourself to the hospital if possible
- Sit down and stay as calm as you can
- Unlock the door if you are alone so emergency responders can enter
- Follow emergency instructions from medical personnel
Do not wait to see whether symptoms improve. Even if symptoms seem mild or come and go, a delay in treatment can increase the amount of heart muscle damage.
Diagnosis
Only EKG can confirm a STEMI within minutes of a patient arriving at the emergency department, or even in the ambulance. This rapid diagnosis is what allows hospitals to activate their cardiac catheterization teams immediately.
Blood tests for cardiac enzymes (troponin) confirm that heart muscle damage has occurred. However, troponin levels may take hours to rise, so treatment for a STEMI is initiated based on the EKG pattern before waiting for blood results.
A coronary angiogram (cardiac catheterization) is typically performed during the emergency treatment itself.
Treatment
Primary percutaneous coronary intervention (PCI) is the gold standard treatment for STEMI. During this procedure, a catheter is guided to the blocked artery, a balloon is inflated to open it, and a stent is placed to keep it open.
Most modern stents are drug-eluting, meaning they release medication over time to prevent the artery from re-narrowing.
Before and during the procedure, patients receive aspirin (to reduce clotting), heparin (to prevent new clots), and often a second antiplatelet agent such as clopidogrel or ticagrelor.
When PCI is not available within the recommended timeframe, for example, in rural areas without a catheterization lab, thrombolytic therapy (clot-dissolving medication) may be used as a bridge to restore some blood flow while the patient is transferred to a PCI-capable facility.
Surgical Options
Coronary artery bypass graft (CABG) surgery may be recommended when the blockage is too complex for a stent, when multiple arteries are severely blocked, or when the left main coronary artery is involved.
Medications After Treatment
After the acute phase, patients are prescribed a combination of long-term medications to protect the heart and prevent another event. These typically include dual antiplatelet therapy (aspirin plus a P2Y12 inhibitor) to prevent clotting around the stent, statins to lower cholesterol and stabilize remaining plaque, beta-blockers to reduce heart rate and blood pressure, and ACE inhibitors or ARBs to support heart function and reduce strain.
Also Read: heart stent recovery time.
Survival Rates and Prognosis
With prompt treatment, in-hospital survival rates for STEMI now exceed 90%. This represents a significant improvement over previous decades, driven by faster door-to-balloon times, improved stent technology, and better emergency response systems.
Thirty-day mortality rates for STEMI range from approximately 2% to 10%, depending on the severity of the blockage, the amount of heart muscle affected, the patient's age, and the presence of other health conditions such as diabetes or kidney disease.
The most dangerous subtype is a complete blockage of the left anterior descending (LAD) artery, known as a widowmaker, which has the highest mortality when it occurs outside a hospital setting.
Complications of STEMI
Because a STEMI causes a portion of heart muscle to lose blood supply entirely, complications can develop during the attack itself, in the days following treatment, or weeks to months into recovery. Most patients who receive prompt PCI do well, but understanding the possible complications helps survivors and their families recognize warning signs early.
Cardiogenic shock
It is the most serious early complication. It occurs in approximately 5 to 8% of STEMIs and develops when the damaged heart muscle can no longer pump enough blood to support the body's organs. Despite advances in treatment, cardiogenic shock still carries a mortality rate approaching 50% and accounts for a disproportionate share of STEMI deaths. It is most often associated with large anterior STEMIs, including widowmaker heart attacks.
Arrhythmias
These are common in the first 24 to 48 hours after a STEMI. These include ventricular tachycardia and ventricular fibrillation, both of which can cause sudden cardiac arrest, as well as atrial fibrillation and conduction abnormalities such as heart block. This is why STEMI patients are monitored in a cardiac care unit immediately after treatment, where any abnormal rhythm can be addressed quickly.
Heart failure
Heart failure can develop when the infarct damages enough muscle to reduce the heart's pumping ability. This is measured by the ejection fraction, which reflects the percentage of blood pumped out of the left ventricle with each beat. A reduced ejection fraction after a STEMI is one of the strongest predictors of long-term outcomes and often requires ongoing medication, lifestyle changes, and close follow-up.
Mechanical complications
These are rare but serious. These include rupture of the papillary muscle (which can cause severe mitral regurgitation), ventricular septal rupture, and free wall rupture.
Pericarditis
It can occur in the days or weeks after a STEMI, caused by inflammation of the sac surrounding the heart. It typically presents as sharp chest pain that worsens when lying flat and improves when sitting forward. Most cases resolve with anti-inflammatory medication.
Left ventricular thrombus
Thrombus can form when blood pools in an area of the heart that is no longer contracting normally, particularly after a large anterior STEMI. If a clot dislodges, it can cause a stroke. Patients identified with LV thrombus on imaging are typically treated with anticoagulation for several months.
Recurrent heart attack and stent thrombosis
These remain as a long-term risk. This is why dual antiplatelet therapy, statins, and risk-factor control are so important after a STEMI. The first 12 months carry the highest risk, and adherence to medication during this period is one of the strongest predictors of avoiding a second event.
Most of these complications are far less common today than they were before the routine use of primary PCI, but recognizing the warning signs, sudden shortness of breath, recurrent chest pain, palpitations, fainting, leg swelling, or unexplained fatigue, can be the difference between early intervention and a serious setback.
Recovery After a STEMI
Most STEMI patients spend two to five days in the hospital after treatment. The general recovery timeline is approximately eight weeks, though individual circumstances vary. Some patients return to desk jobs within two to three weeks, while those with physically demanding work or significant heart damage may need up to three months.
Driving is typically restricted for one to two weeks, and strenuous activity is gradually reintroduced under medical guidance.
Cardiac Rehabilitation
Cardiac rehabilitation is one of the most impactful steps a STEMI survivor can take. The CDC reports that completing a cardiac rehab program reduces cardiovascular death risk by nearly 45% and hospital readmissions by approximately 30%.
Fewer than 15% of eligible patients in the United States complete cardiac rehabilitation. Transportation challenges, scheduling conflicts, and limited access to facilities are among the most common barriers.
Carda Health's virtual cardiac rehab program removes these barriers by delivering supervised, at-home rehabilitation sessions with a clinical exercise physiologist who monitors vital signs in real time. The program also includes nutrition, stress management, and ongoing education. For STEMI survivors, completing a full rehab program from home can be the difference between a strong recovery and an incomplete one.
Also Read: Does Medicare Cover Pulmonary Rehabilitation
Emotional recovery matters too. Depression and anxiety are common after a STEMI, affecting up to one in three survivors. Left unaddressed, these conditions can undermine medication adherence, reduce physical activity, and worsen cardiac outcomes. A comprehensive rehab program that includes psychosocial support helps address these challenges as part of the overall recovery plan.
{{get-started}}
FAQs
What is a STEMI heart attack?
A STEMI (ST-elevation myocardial infarction) is a severe type of heart attack caused by a complete blockage of a coronary artery. The blockage stops blood flow entirely to a portion of the heart muscle, causing tissue to die.
Is a STEMI the worst type of heart attack?
A STEMI is generally considered the most dangerous type of heart attack because the coronary artery is completely blocked, meaning no blood is reaching the affected heart muscle. However, outcomes depend heavily on how quickly treatment is received. A STEMI treated in hospital within 60 to 90 minutes can result in relatively limited damage, while a less severe heart attack that goes untreated for hours can be far more harmful.
What is the survival rate of a STEMI?
With prompt hospital treatment (primary PCI), in-hospital survival rates for STEMI exceed 90%. Thirty-day mortality ranges from approximately 2% to 10% depending on severity and comorbidities. The widowmaker subtype, a complete blockage of the LAD artery, has the highest mortality when it occurs outside a hospital (~12% survival), but also exceeds 90% survival with prompt in-hospital PCI.
What is the difference between STEMI and NSTEMI?
A STEMI involves a complete blockage of a coronary artery, while an NSTEMI involves a partial blockage with some blood flow still reaching the heart. On an EKG, a STEMI shows ST-segment elevation; an NSTEMI does not. Both cause heart muscle damage (elevated troponin), but a STEMI is treated with more urgency because the artery is fully occluded.
References
- Cleveland Clinic. STEMI: Causes, Treatment & Outlook.
- Mechanic OJ, Gavin M, Engel A. Acute Myocardial Infarction (STEMI). StatPearls. 2024.
- O'Gara PT, et al. 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction. Circulation. 2013;127(4).
- Thygesen K, Alpert JS, et al. Fourth Universal Definition of Myocardial Infarction. Circulation. 2018;138(20).
- American Heart Association. Heart Attack and Stroke Statistics.
- Centers for Disease Control and Prevention. Cardiac Rehabilitation.


