

Key Takeaways
- Cervical angina is chest pain that closely mimics cardiac angina but originates from disorders of the cervical spine (neck), not from the heart.
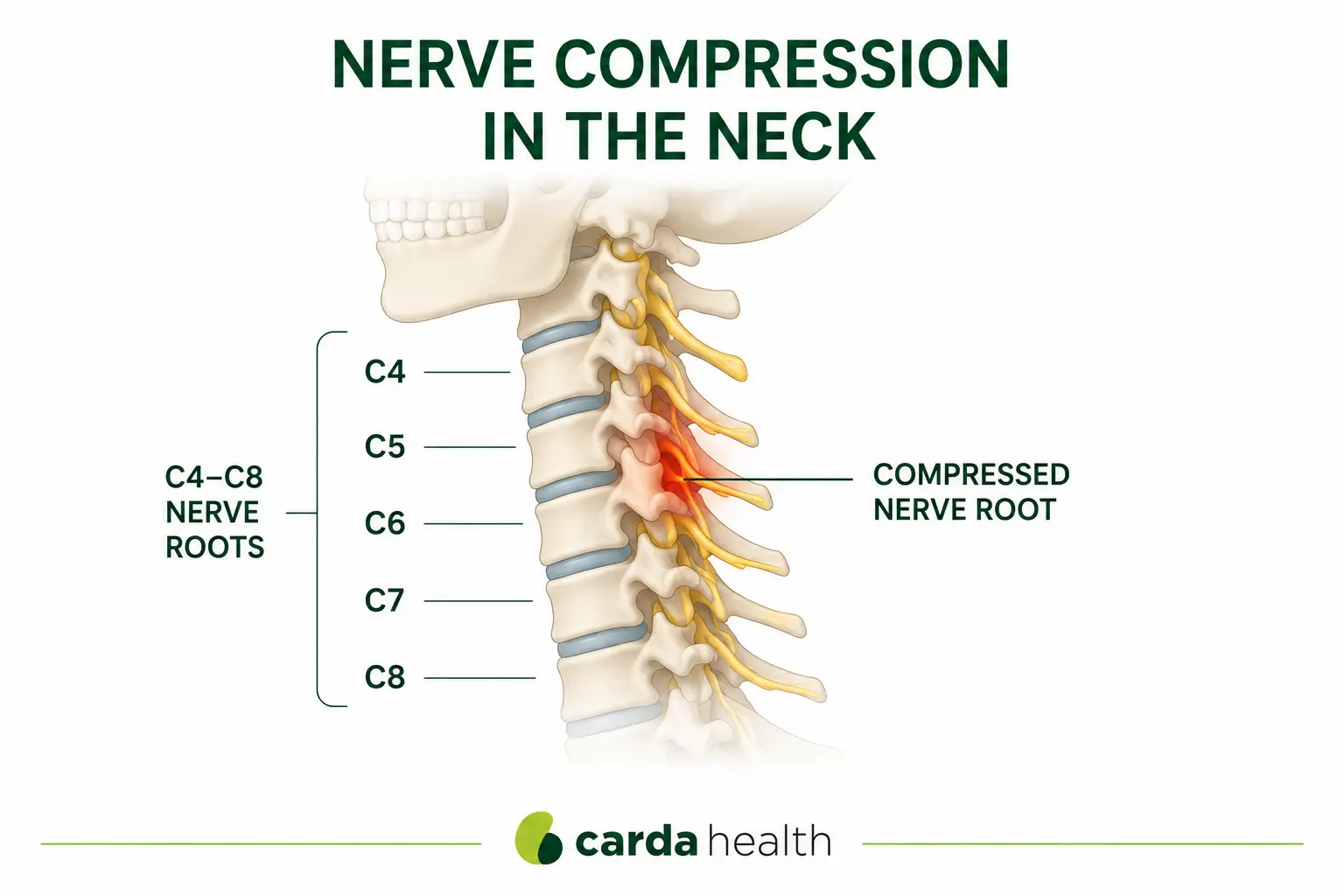
- It is most commonly caused by nerve root compression at the C4-C8 levels.
- Cervical angina is not dangerous to the heart, but cardiac causes must always be ruled out first.
- Once diagnosed, most patients respond well to conservative treatment including physical therapy, medication, and lifestyle modifications.
What Is Cervical Angina?
Cervical angina, also called pseudoangina or cervicogenic angina, is chest pain that feels remarkably similar to the chest pain caused by heart disease, but actually originates from problems in the cervical spine (neck). The pain can be sharp, aching, or crushing, and may radiate to the arm, shoulder, or jaw, the same pattern that occurs during a heart attack or cardiac angina.
This matters because more than half of the patients who present to emergency departments with chest pain do not have a cardiac cause. Cervical angina is one of the potential noncardiac explanations that is frequently overlooked, leaving patients anxious, frustrated, and without effective treatment.
What Causes Cervical Angina?
The exact mechanisms are still being studied, but research has identified several pathways through which cervical spine disorders can produce chest pain.
Approximately 70% of cervical angina cases are attributed to compression of the C4 through C8 nerve roots, according to a comprehensive review published in the Asian Spine Journal.
Symptoms of Cervical Angina
The hallmark of cervical angina is that it closely mimics cardiac chest pain, which is precisely what makes it so difficult to diagnose.
Some patients also experience autonomic symptoms such as shortness of breath, nausea, dizziness, sweating, or heart palpitations. These symptoms can make cervical angina even more frightening and more difficult to distinguish from a true cardiac event without proper testing.
{{get-started}}
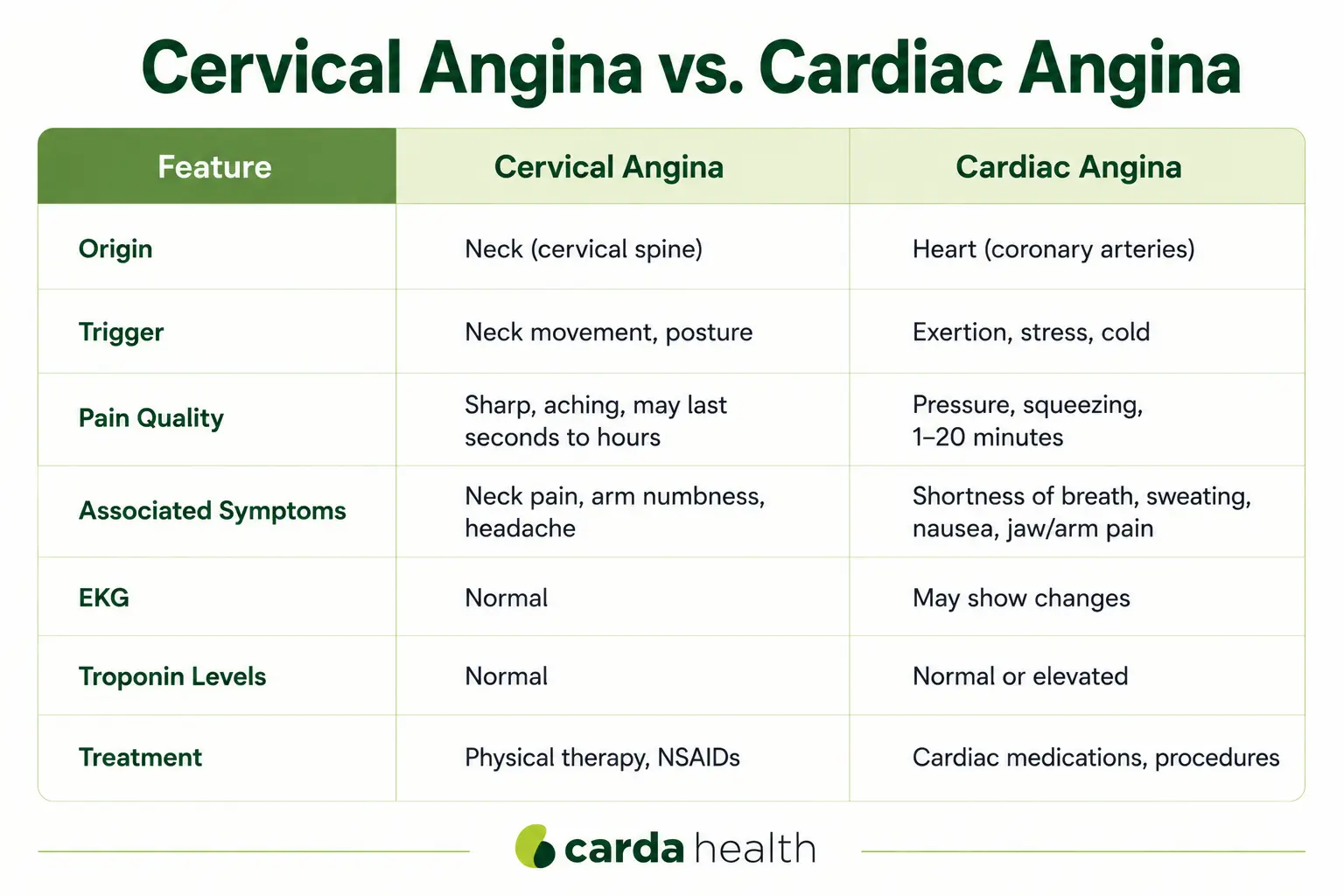
Cervical Angina vs. Cardiac Angina
Because cervical angina so closely mimics true cardiac angina, understanding the distinguishing features is essential. The table below highlights the key differences.
How Cervical Angina Is Diagnosed
Cervical angina is a diagnosis of exclusion, meaning cardiac causes must be thoroughly ruled out before the cervical spine is considered as the source of chest pain. This is a critical point. Chest pain should always be treated as a potential cardiac emergency until proven otherwise.
First, a complete cardiac workup is performed, which may include an electrocardiogram (EKG), blood tests for cardiac enzymes (troponin), stress testing, and in some cases a coronary angiogram. If all cardiac tests are negative, the evaluation moves to the next step.
Second, a neurologic examination is performed. One of the most revealing clinical tests is the Spurling maneuver.
Third, cervical imaging confirms the diagnosis. MRI of the cervical spine is the preferred imaging study and may reveal herniated discs, foraminal stenosis, spinal cord compression, or degenerative changes. CT imaging can show bony overgrowths at the Luschka's joints that may be contributing to nerve compression.
Treatment
The majority of patients with cervical angina respond well to conservative (non-surgical) treatment. First-line approaches include nonsteroidal anti-inflammatory drugs (NSAIDs) to reduce pain and inflammation.
Physical therapy is particularly important because it addresses the underlying mechanical problems, poor posture, muscle imbalance, and reduced cervical mobility, that contribute to nerve compression.
When Surgery May Be Needed
Surgery is considered when conservative treatment fails to provide adequate relief after at least three months, or when there is evidence of neurologic compromise such as progressive weakness or signs of spinal cord compression (myelopathy). The most common surgical approach is anterior cervical discectomy and fusion (ACDF), which removes the damaged disc and fuses the affected vertebrae to stabilize the spine.
Important Note: Rule Out Cardiac Causes
This point cannot be emphasized enough: cervical angina is a diagnosis that can only be made after cardiac disease has been thoroughly excluded. Some patients may have both cervical spine problems and coexisting cardiac risk factors. The two conditions are not mutually exclusive.
If you are experiencing chest pain of any kind, seek emergency medical evaluation. Do not attempt to self-diagnose based on the presence of neck symptoms.
Also Read: what happens after a heart attack
If your cardiac evaluation does reveal coronary artery disease, heart failure, or another cardiac condition, structured rehabilitation can play an important role in your recovery. Carda Health's virtual cardiac rehab program provides supervised exercise, nutritional guidance, and ongoing education from home, learn more in our guide to cardiac rehabilitation.
{{get-started}}
FAQs
Can neck problems really cause chest pain?
Yes. The nerve roots that exit the cervical spine at the C4 through C8 levels supply sensory and motor innervation to the anterior chest wall. When these nerves are compressed or irritated by disc herniations, bone spurs, or spinal stenosis, the resulting pain can be felt in the chest, arm, shoulder, or jaw, closely mimicking a heart attack.
What is the difference between cervical angina and a heart attack?
A heart attack is caused by blocked blood flow to the heart muscle and is a life-threatening emergency. Cervical angina is caused by nerve compression in the neck and is not dangerous to the heart. However, the symptoms can feel nearly identical, which is why cardiac causes must always be ruled out first through proper medical testing.
Is cervical angina dangerous?
Cervical angina is not dangerous to the heart. However, the chest pain it causes can be severe and significantly affect quality of life. The condition can also cause anxiety and depression due to the uncertainty of living with unexplained chest pain.
Can cervical angina be cured?
Many patients experience complete resolution of symptoms with conservative treatment including physical therapy, anti-inflammatory medications, and cervical traction.
References
- Christensen N, Searle R, Bhatt D. Cervical Angina: An Overlooked Source of Noncardiac Chest Pain. J Hosp Med. 2014. PMC4272356.
- Feng F, Chen X, Shen H. Cervical Angina: A Literature Review on Its Diagnosis, Mechanism, and Management. Asian Spine J. 2021;15(4):550-556. PMC8377215.
- Al Jammal O, et al. Cervical Angina as a Cause of Non-Cardiac Chest Pain: A Case Report. J Med Case Rep. 2023. PMC10103829.
- Feng F, et al. Different Surgical Strategy for Patients With Cervical Angina: A Potential Role of Luschka's Joint Osteophyte. Orthop Surg. 2020;12(4):1211-1218.
- National Heart, Lung, and Blood Institute (NHLBI). Angina - Types. nhlbi.nih.gov/health/angina/types.
{{get-started}}


