

Key Takeaways
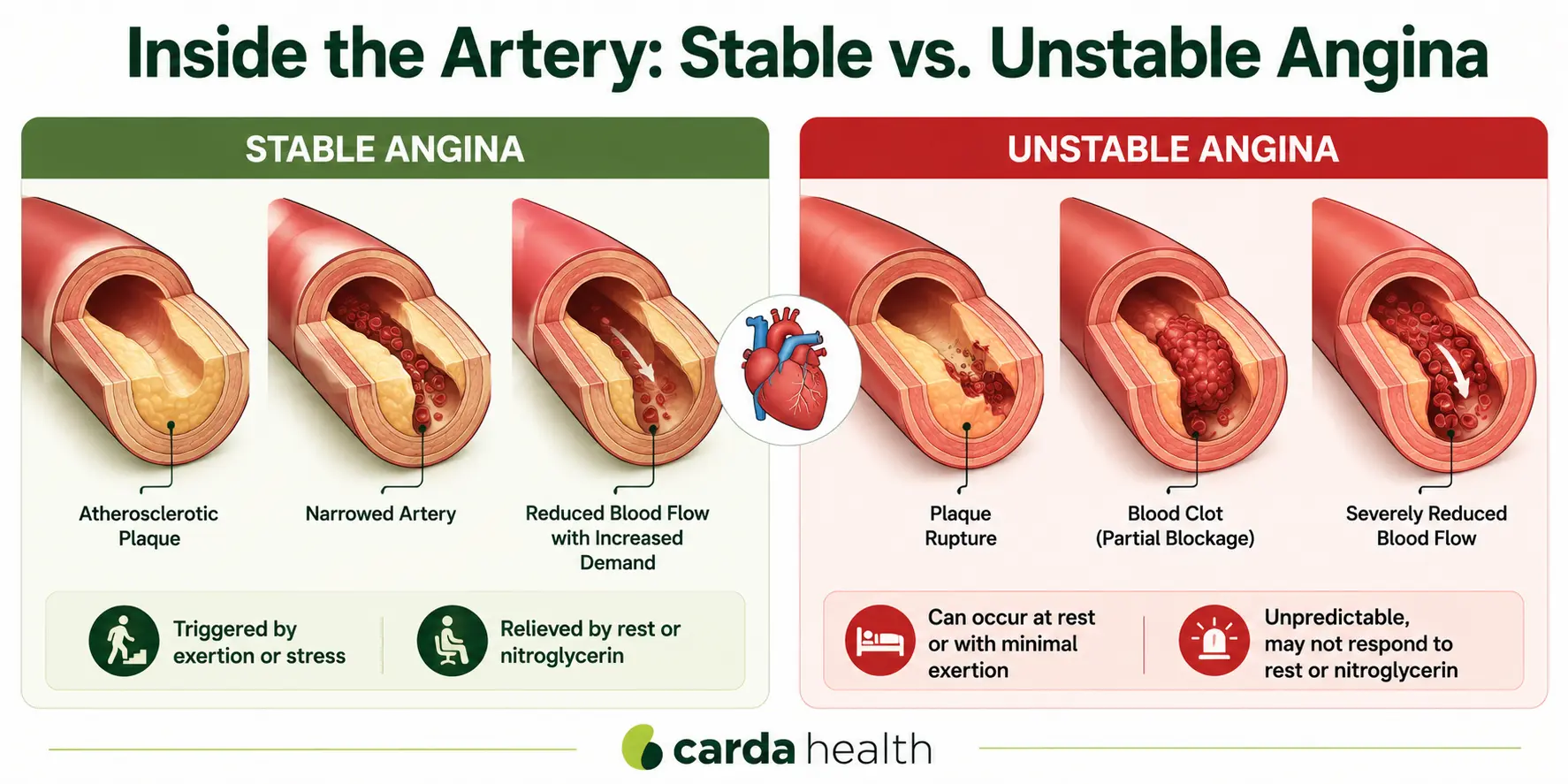
- Stable angina follows a predictable pattern, it typically occurs during physical exertion or stress and improves with rest or nitroglycerin.
- Unstable angina is unpredictable, can occur at rest, lasts longer, and may not respond to medication.
- Unstable angina is a medical emergency and a warning sign of an imminent heart attack.
- Knowing the difference can save your life.
What Is Angina?
Angina is often described as a feeling of pressure, tightness, squeezing, or heaviness in the chest. It may also radiate to the arms, shoulders, jaw, neck, or back. Understanding the type of angina you are experiencing is essential because the two main forms, stable and unstable, carry very different levels of risk and require different responses.
What Is Stable Angina?
Stable angina, the most common form of angina, follows a predictable, recognizable pattern, meaning you can generally anticipate when it will occur, what will trigger it, and how to relieve it. While stable angina signals that coronary artery disease is present, it is considered manageable with the right combination of medication, lifestyle changes, and medical monitoring.
How It Feels
The most common sensation is chest pressure or tightness, often described as a weight or squeezing feeling in the center of the chest. The discomfort may spread to the left arm, jaw, neck, shoulders, or upper back. Some patients also experience shortness of breath, fatigue, or a mild burning sensation. Episodes typically last between one and five minutes, and rarely exceed 15 minutes.
What Triggers It
Stable angina is triggered by situations that increase the heart's demand for oxygen. The most common triggers include physical exertion (exercise, climbing stairs, heavy lifting), emotional stress, cold weather, and eating a large meal.
What Relieves It
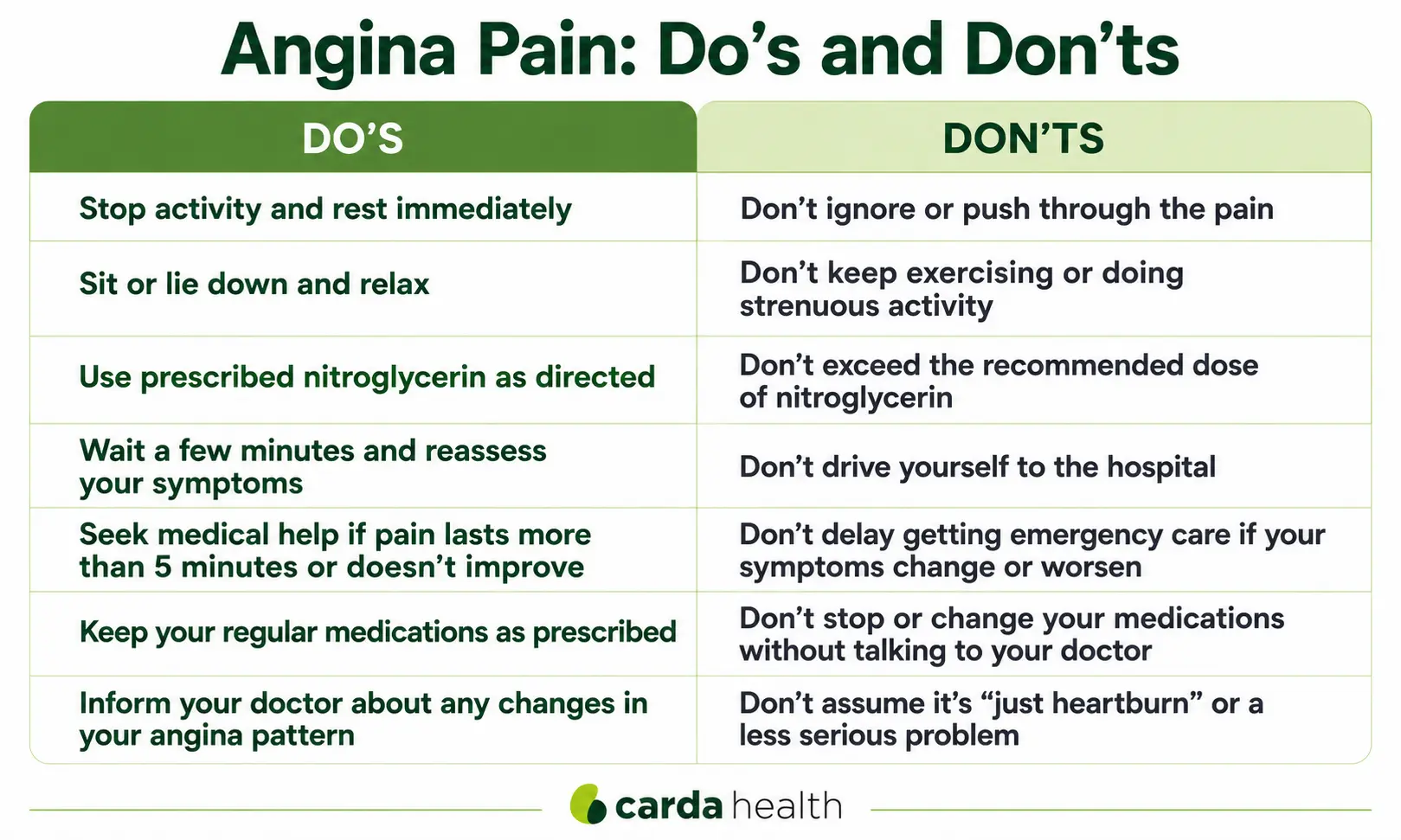
The hallmark of stable angina is that it responds to rest and nitroglycerin. Stopping the triggering activity and sitting or lying down usually allows the pain to subside within a few minutes. A sublingual nitroglycerin tablet or spray provides additional relief by widening the coronary arteries and improving blood flow.
If the pain does not ease within five minutes after nitroglycerin, or if the pattern changes, it is time to seek medical attention, the angina may be becoming unstable.
{{get-started}}
What Is Unstable Angina?
Unlike stable angina, unstable angina does not follow a predictable pattern. It can occur without any clear trigger, at rest, during sleep, or with minimal exertion. The pain tends to be more intense, lasts longer (often 20 minutes or more), and may not respond to rest or nitroglycerin.
Clinically, unstable angina is recognized when chest pain meets any one of three patterns:
Rest angina: chest pain occurring at rest, typically lasting longer than 20 minutes.
New-onset severe angina: chest pain that has appeared within the past two months and is significant enough to limit normal activity.
Crescendo angina: a previously stable pattern that has now become more frequent, more severe, longer-lasting, or triggered by less exertion than before.
Any one of these is enough to classify the angina as unstable. You do not need all three, and the episode does not have to last 20 minutes always if it represents a new or worsening pattern. This is why a change in your usual angina, even a subtle one, is taken seriously by cardiologists.
Why It's an Emergency
Unstable angina is classified as an acute coronary syndrome (ACS), the same category that includes heart attacks. According to the American Heart Association, unstable angina should always be treated as a medical emergency because it indicates that a plaque in a coronary artery has ruptured or eroded, and a blood clot is partially blocking blood flow. Without treatment, this partial blockage can quickly become a complete blockage, resulting in a heart attack.
Clinical Distinction Between Unstable Angina and a Heart Attack
Troponin levels in the lab results distinguish both. In unstable angina, troponin levels stay below the threshold used to diagnose a heart attack. In an NSTEMI (heart attack), troponin is elevated, indicating that some heart tissue has begun to die.
This is why emergency blood tests are so critical.
Read more: Angina vs Heart Attack
Stable vs. Unstable Angina: Key Differences at a Glance
Also read: What happens when a coronary artery becomes fully blocked?
How Symptoms Can Differ by Sex and Age
The classic description of angina, central chest pressure radiating to the left arm, fits many patients but not all. Women, adults over 65, and people with diabetes are more likely to experience symptoms that don't match the textbook picture. These can include unusual fatigue, shortness of breath, jaw or upper back discomfort, nausea, or a vague sense of being unwell, sometimes without prominent chest pain at all.
Current cardiology guidelines have moved away from labeling these presentations as "atypical" because for these populations, they are typical. If you have risk factors for coronary disease and are experiencing new or unexplained symptoms that feel like they could be coming from your heart, take them seriously even if they don't match the standard description.
Diagnosis
Determining whether chest pain is caused by stable angina, unstable angina, or another condition requires a systematic evaluation. Your doctor will use a combination of your symptom history, physical examination, and targeted testing.
Electrocardiogram (EKG) is typically the first test. In stable angina, the resting EKG may appear normal, which is why stress testing is often the next step.
Blood tests measure cardiac biomarkers, particularly high-sensitivity troponin. In unstable angina, troponin levels remain below the threshold for heart muscle damage. In an NSTEMI, troponin is elevated.
Stress testing (exercise or pharmacologic) evaluates how the heart responds to increased demand. If you cannot exercise, a medication-induced stress test with imaging (nuclear or echocardiographic) can provide similar information.
Coronary angiogram (cardiac catheterization) is the definitive imaging study. It uses contrast dye and real-time X-ray to visualize the exact location and severity of arterial blockages. For more on this procedure, see our article on what is an angiogram.
Treatment
Managing Stable Angina
Stable angina is managed with a combination of medication, lifestyle changes, and ongoing monitoring. Nitroglycerin provides acute relief during episodes. Long-term medications typically include beta-blockers (to reduce heart rate and oxygen demand), calcium channel blockers (to widen arteries), long-acting nitrates (to prevent episodes), statins (to lower cholesterol and stabilize plaque), and low-dose aspirin (to reduce clotting risk).
If medications and lifestyle changes are not sufficient to control symptoms, revascularization may be recommended. This typically involves either percutaneous coronary intervention (angioplasty with stent placement) or coronary artery bypass graft (CABG) surgery.
Treating Unstable Angina
Unstable angina requires emergency treatment. Patients are typically hospitalized for continuous cardiac monitoring and stabilization. Immediate medications include aspirin, a second antiplatelet agent (such as clopidogrel or ticagrelor), intravenous heparin to prevent further clotting, nitroglycerin to improve blood flow, and beta-blockers to reduce the heart's workload. Statins are also started early.
In many cases, urgent cardiac catheterization is performed to evaluate the blockage, and angioplasty with stenting is done during the same procedure to restore blood flow. For severe or multi-vessel disease, CABG surgery may be needed. After the acute phase, recovery follows a similar path to heart attack recovery, including cardiac rehabilitation. For more on what to expect, see our guide on heart stent recovery time.
Cardiac Rehabilitation for Angina
Cardiac rehabilitation is relevant for both forms of angina. Stable angina is a Medicare-covered qualifying diagnosis for cardiac rehab. A structured rehab program combines supervised exercise training, education on heart-healthy living, nutritional guidance, and stress management, all of which directly address the underlying coronary artery disease that causes angina.
Carda Health's virtual cardiac rehab program makes it possible to complete a full rehabilitation program from home. Each session is supervised by a clinical exercise physiologist who monitors vital signs in real time, ensuring safe and effective exercise progression.
The program also includes the Ornish Lifestyle Medicine program, the only program scientifically proven to reverse heart disease through comprehensive lifestyle changes.
Learn more in our guides on benefits of cardiac rehabilitation and virtual cardiac rehab.
When to Call 911 vs. When to See Your Doctor
Call 911 immediately if: you experience chest pain for the first time and have never been evaluated, your usual angina pattern changes (more frequent, more intense, triggered by less activity, or occurring at rest), chest pain lasts more than five minutes and does not improve with nitroglycerin (after up to three doses spaced five minutes apart), or you experience additional symptoms such as shortness of breath, sweating, nausea, lightheadedness, or pain spreading to the arm, jaw, or back.
Schedule a doctor visit if: you have mild, predictable chest discomfort with exertion that reliably resolves with rest, you want to be evaluated for coronary artery disease risk factors, or you want to review your current angina management plan and medications with your cardiologist.
What happens if you have a heart attack and don't go to the hospital?
How to Reduce Your Risk of Unstable Angina
Managing blood pressure, cholesterol, and blood sugar through regular monitoring and medication adherence is essential. Quitting smoking at any age significantly reduces cardiovascular risk. Staying physically active, eating a heart-healthy diet while limiting saturated fats, sodium, and added sugars supports arterial health. Managing stress through relaxation techniques, social connection, and adequate sleep also helps.
Read our guide on exercises after a heart attack.
Conclusion
Angina is your heart's way of telling you that it is not getting enough blood. Stable angina gives you a consistent, recognizable warning, one that you can manage with medication, lifestyle changes, and cardiac rehabilitation. Unstable angina is an urgent alarm that demands immediate emergency care.
For patients living with stable angina or recovering after unstable angina treatment, cardiac rehabilitation provides the structured support that improves heart function, reduces future risk, and restores confidence in daily activity.
{{get-started}}
Frequently Asked Questions
What is the main difference between stable and unstable angina?
Stable angina follows a predictable pattern, it is triggered by exertion or stress and relieves with rest or nitroglycerin within a few minutes. Unstable angina is unpredictable, it can occur at rest, lasts longer (often 20+ minutes), and may not respond to nitroglycerin. Unstable angina is a medical emergency.
Can stable angina turn into unstable angina?
Yes. If the underlying coronary artery disease worsens, for example, if a plaque grows or partially ruptures, stable angina can progress to unstable angina. Warning signs include episodes that are more frequent, triggered by less activity, last longer, or occur at rest.
Is unstable angina the same as a heart attack?
Not exactly, but they are closely related. Both are classified as acute coronary syndromes. The key difference is that in unstable angina, troponin levels stay below the threshold used to diagnose a heart attack (no heart muscle damage has occurred yet), while in a heart attack (NSTEMI), troponin is elevated, indicating cell death. Unstable angina can quickly progress to a heart attack without treatment.
How long does an unstable angina episode last?
Unstable angina episodes typically last 20 minutes or longer. Unlike stable angina, the pain may not subside with rest or nitroglycerin. Any chest pain lasting more than five minutes that does not respond to nitroglycerin should be treated as a potential emergency.
What should I do if my angina pattern changes?
Call 911. Treat any change in your angina pattern as urgent. If pain is becoming more frequent, lasting longer, occurring with less exertion, or happening at rest, seek medical attention right away.
Can you exercise with stable angina?
Yes, with proper medical guidance. Regular physical activity is actually recommended for people with stable angina because it improves cardiovascular fitness and can reduce the frequency of episodes over time.
Is cardiac rehab recommended for angina?
Yes. Stable angina is a qualifying diagnosis for cardiac rehabilitation (covered by Medicare and most insurance plans). Cardiac rehab is also standard care after treatment for unstable angina. Programs include supervised exercise, education, nutrition counseling, and stress management, all of which directly address the coronary artery disease that causes angina.
References
- National Heart, Lung, and Blood Institute (NHLBI). Angina, Types. nhlbi.nih.gov/health/angina/types.
- American Heart Association. Unstable Angina. heart.org.
- Braunwald E, et al. ACC/AHA Guidelines for the Management of Patients With Unstable Angina and Non-ST-Segment Elevation Myocardial Infarction. Circulation. 2000;102(10):1193-1209.
- StatPearls. Unstable Angina. National Center for Biotechnology Information. ncbi.nlm.nih.gov/books/NBK442000.
- Maron DJ, et al. Initial Invasive or Conservative Strategy for Stable Coronary Disease (ISCHEMIA). N Engl J Med. 2020;382:1395-1407.
- Boden WE, et al. Evaluation and Management of Patients With Stable Angina: Beyond the Ischemia Paradigm. JACC. 2021;78(20):2022-2038.
- MedlinePlus. Unstable Angina. medlineplus.gov/ency/article/000201.htm.
- Mayo Clinic. Angina, Symptoms and Causes. mayoclinic.org.
- Centers for Disease Control and Prevention. Cardiac Rehabilitation. cdc.gov.


