Telehealth Cardiac and Pulmonary Rehab in 2026: What the New Rules Mean for Providers
.avif)

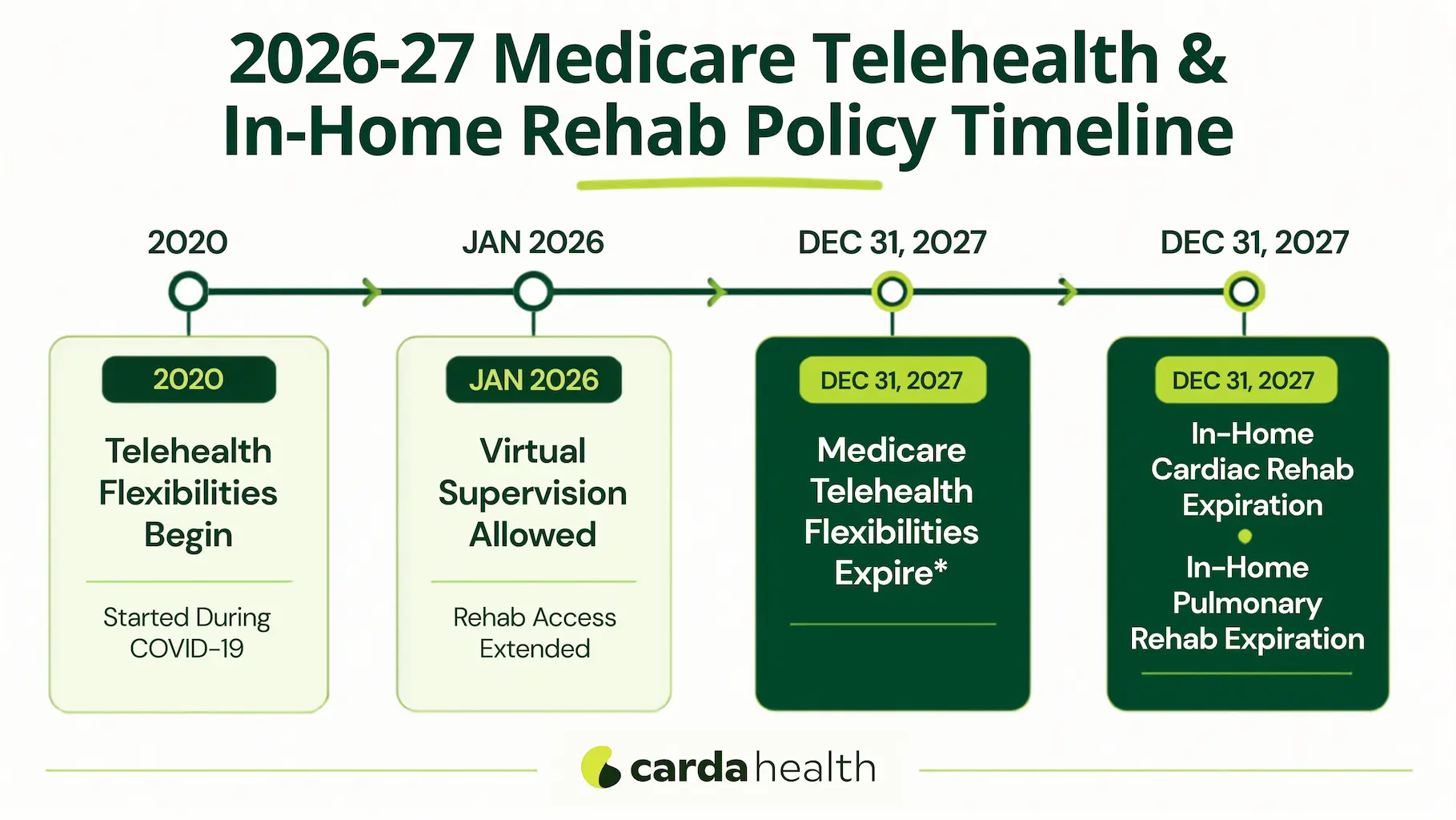
Key Takeaways: Two 2026 policy changes expanded virtual cardiac and pulmonary rehabilitation. The CMS 2026 Physician Fee Schedule permanently lets clinicians supervise rehab virtually and adds cardiac and pulmonary rehab to the Medicare telehealth list for physician office-based programs. The Consolidated Appropriations Act, 2026, signed February 3, 2026, goes further: it lets Medicare patients complete cardiac and pulmonary rehab at home via telehealth, including through hospital outpatient programs, through December 31, 2027, the same date through which it extends general Medicare telehealth flexibilities. For providers, this is a time-limited window to expand access, capacity, and reimbursed virtual programs.
If you run a cardiac or pulmonary rehabilitation program, 2026 brought some of the most consequential policy changes in years, and also some of the most confusing. Two separate developments, one regulatory and one legislative, reshaped what "virtual rehab" can mean and how it gets paid. They are easy to mix up, and most coverage online blends them together.
This guide explains the two changes in plain language, explains what they mean for office-based and hospital-based programs, and lays out why now is the moment to build or expand a virtual program.
The 2026 Updates at a Glance
What Changed? Two Parallel Changes in Telehealth
The simplest way to think about 2026 is two tracks running side by side. One came from CMS through its annual payment rule; the other came from Congress through a funding bill. They overlap, but they are not the same.
The CMS 2026 Rule: Permanent Virtual Supervision
On October 31, 2025, CMS finalized its calendar year 2026 Physician Fee Schedule, effective January 1, 2026. Two parts matter for rehab. First, CMS made virtual direct supervision permanent: a supervising physician or qualified non-physician practitioner can now be "present" through real-time, two-way audio-video technology rather than physically on-site, for cardiac rehabilitation (CR), intensive cardiac rehabilitation (ICR), and pulmonary rehabilitation (PR).
For physician offices, this authority comes from the CY2026 Physician Fee Schedule; for hospital outpatient departments, the companion CY2026 OPPS final rule adopts the same permanent virtual-supervision policy. Together they apply across both settings, and it is a meaningful answer to staffing and workforce pressures.
Second, CMS permanently added CR, ICR, and PR to the Medicare Telehealth Services List, but only for physician office-based programs. These services must be delivered with real-time, continuous audio-video technology; audio-only does not qualify. Crucially, hospital outpatient departments were left out, and could not deliver rehab to the home under the statute. Fixing that required Congress.
The Consolidated Appropriations Act, 2026: In-Home Rehab Extended
That fix arrived quickly. The Consolidated Appropriations Act, 2026 (H.R. 7148) passed the House on January 22 and was signed into law on February 3, 2026. As the American College of Cardiology summarized, the package extended Medicare telehealth flexibilities and reestablished in-home cardiac and pulmonary rehabilitation services, both through December 31, 2027.
According to an American Action Forum analysis of the law, a dedicated section lets Medicare patients receive cardiopulmonary rehabilitation at home or via telehealth, temporarily waiving the requirement that they be physically present in an outpatient facility. In practice, that closes the hospital-outpatient gap the CMS rule left open, so both office-based and hospital-based programs can deliver rehab to the home through the end of 2027.
{{get-started}}
Why the Office-Based vs. Hospital (HOPD) Distinction Matters
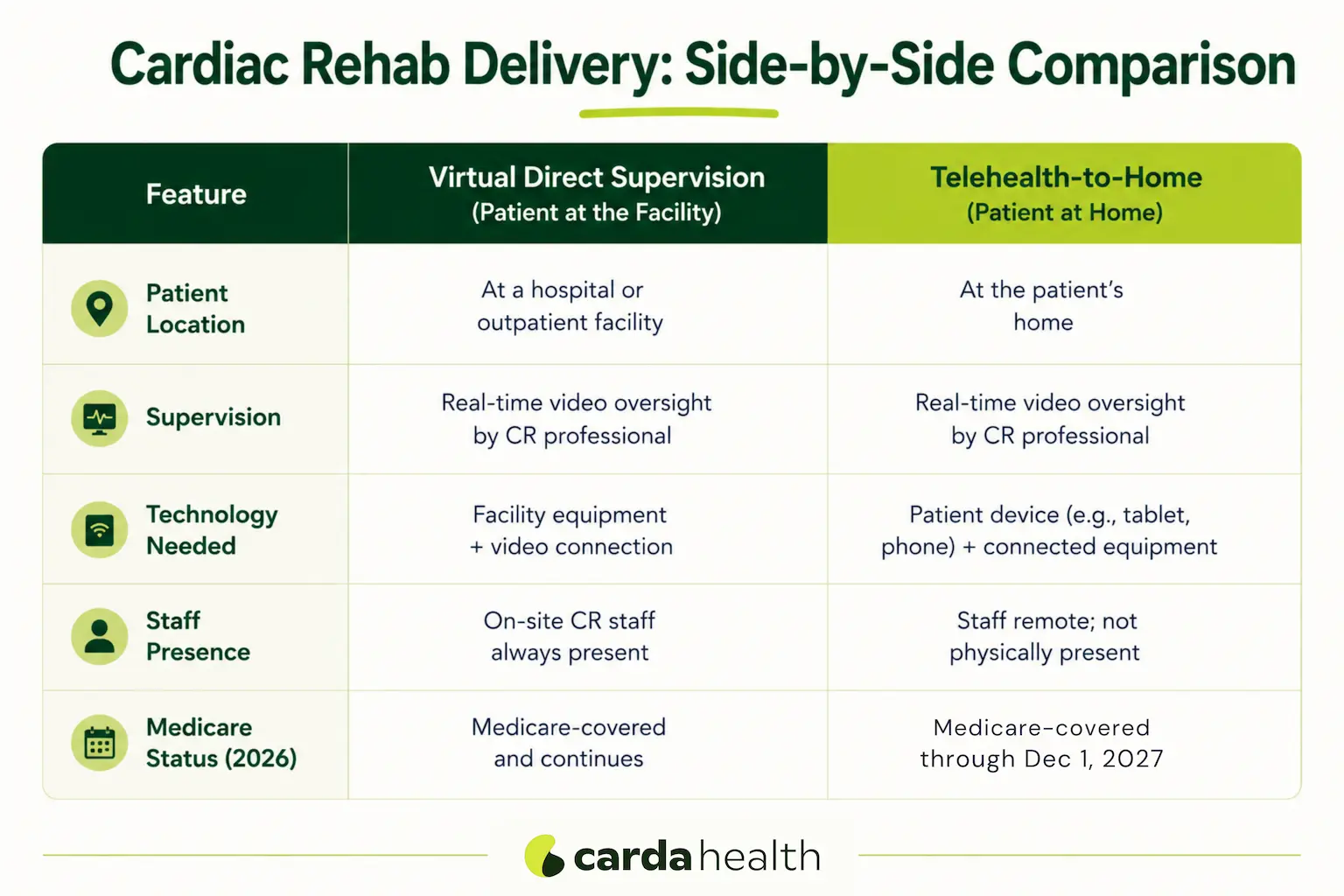
There are two different ideas hiding behind the phrase "virtual rehab."
- Virtual supervision means the patient is still physically in the rehab facility, but the supervising clinician joins by live video. The CMS rule made this permanent for both office and hospital programs.
- Telehealth-to-home means the patient does rehab from home and connects by live video. The CMS rule allowed this permanently for office-based programs only; the Consolidated Appropriations Act, 2026 temporarily extended it to hospital-based programs too, through Dec 31, 2027.
Because the large majority of cardiac and pulmonary rehab in the United States is delivered by hospital outpatient departments, the congressional extension is what actually lets most programs send rehab into patients' homes. For a deeper look at how these delivery models compare, see our guide to the best cardiac rehab treatment models in 2026.
How Virtual Cardiac and Pulmonary Rehab Is Reimbursed?
Reimbursement follows the same session-based logic as in-person rehab, using the established cardiac rehab codes (such as 93797 and 93798), intensive cardiac rehab codes (G0422 and G0423), and the pulmonary rehab code (G0424), delivered under the telehealth and supervision rules above. Many programs also layer in remote physiologic monitoring (CPT 99453-99458) to support virtual care between sessions. These codes are defined in the CMS Medicare Physician Fee Schedule and HCPCS Level II coding guidance, with rehab-specific billing detail available from the AACVPR.
Two practical notes. First, the new law directs HHS to create unique billing codes or modifiers when a provider uses a third-party telehealth platform, so documentation and platform transparency will matter more going forward. Second, pulmonary rehab coverage at home remains more nuanced than cardiac rehab; we break down the specifics in our guide on whether Medicare covers pulmonary rehab. As always, programs should confirm current CMS guidance and individual payer policies before billing.
Why Providers Should Act Now
Policy windows like this don't stay open forever, and the case for building virtual rehab capacity is about far more than a billing opportunity.
The Cardiac Rehab Access and Completion Gap
Cardiac rehabilitation is one of the most strongly recommended interventions in cardiology, a guideline-backed therapy shown to reduce hospital readmissions and mortality after a cardiac event. Yet it is dramatically underused. Despite heart disease remaining the leading cause of death in the United States, as the CDC reports, only a minority of eligible patients ever enroll, and many who start never finish. The most common reasons are practical: transportation, distance, scheduling, and the burden of repeated trips to a center.
Telehealth directly targets those barriers. The AACVPR, AHA, and ACC home-based cardiac rehabilitation scientific statement concluded that, for appropriately selected patients, home-based delivery can achieve outcomes comparable to traditional center-based programs while reaching people who would otherwise go without. Removing the commute is often the difference between a patient finishing rehab and dropping out.
Capacity, Outcomes, and Value-Based Care
For administrators, virtual delivery is also a capacity strategy. A home-based program can expand enrollment without the floor space, equipment, and staffing constraints of a physical center, helping programs serve more patients and shorten wait times after discharge. And because rehab improves outcomes and reduces readmissions, stronger participation aligns neatly with value-based and bundled-payment models, where avoiding readmissions has direct financial stakes.
With reimbursement assured only through December 31, 2027, providers who build now have time to stand up programs, demonstrate outcomes, and be well positioned if and when these flexibilities are made permanent. You can review the broader clinical case in our complete guide to cardiopulmonary rehabilitation and the benefits of cardiac rehabilitation.
Bringing Virtual Rehab to Your Patients
Building a virtual program from scratch is a significant undertaking, clinical protocols, remote monitoring equipment, staffing, and payer coordination all have to come together. Carda Health partners with health systems and plans to deliver virtual cardiac and pulmonary rehabilitation directly to patients' homes: supervised sessions over live video, shipped remote-monitoring devices, a dedicated clinician for each patient, and handling of the eligibility and coverage paperwork that often slows enrollment. For many programs, partnering is the fastest way to extend reach into the home while the current reimbursement window is open.
Conclusion
The headline for 2026 is straightforward once the two tracks are separated: virtual supervision of cardiac and pulmonary rehab is now permanent, and delivering rehab to the home by telehealth is broadly available, for both office and hospital programs, through the end of 2027. That combination removes long-standing access barriers, expands capacity, and supports better outcomes for patients who need rehab most.
The window is real but time-limited. Providers who move now can close the access gap for their patients and build durable virtual programs before these flexibilities are reconsidered.
{{get-started}}
Frequently Asked Questions
Is virtual cardiac rehab covered by Medicare in 2026?
Yes. Under the CMS 2026 rule, physician office-based programs can deliver cardiac and pulmonary rehab by telehealth permanently, and the Consolidated Appropriations Act, 2026 lets both office and hospital programs deliver rehab to the home through Dec 31, 2027. Coverage requires real-time, two-way audio-video; audio-only does not qualify.
When do the telehealth cardiac and pulmonary rehab flexibilities expire?
General Medicare telehealth flexibilities run through December 31, 2027. The provision allowing in-home and telehealth cardiac and pulmonary rehab, including for hospital outpatient programs, runs through Dec 31, 2027, unless Congress extends or makes it permanent.
Can hospital outpatient departments offer virtual cardiac rehab?
Now, yes. The CMS rule alone left hospital outpatient departments unable to deliver rehab to the home, but the Consolidated Appropriations Act, 2026 added that authority temporarily, through Dec 31, 2027.
What's the difference between virtual supervision and telehealth-to-home rehab?
Virtual supervision means the patient is still at the facility while a clinician supervises by live video, now permanent. Telehealth-to-home means the patient does rehab from home over live video, permanent for office-based programs and, through the end of 2027, available to hospital programs as well.
Does Medicare cover pulmonary rehab at home?
Through Dec 31, 2027, the new law allows pulmonary rehab to be furnished at home via telehealth alongside cardiac rehab. Coverage details can vary by setting and plan, so confirm current CMS guidance and the patient's specific plan before enrolling.
How is virtual cardiac rehab reimbursed?
It uses the same session-based cardiac and pulmonary rehab codes as in-person care, delivered under the telehealth and supervision rules, and programs often add remote physiologic monitoring. New rules also require billing transparency when a third-party telehealth platform is used.
Will telehealth cardiac rehab become permanent?
Virtual supervision is already permanent. The in-home/telehealth delivery flexibilities are currently temporary, and professional groups continue to advocate for a permanent fix through legislation such as the Sustainable Cardiopulmonary Rehabilitation Services in the Home Act.
References
- American College of Cardiology. Congress Passes Critical Health Program Funding, Extends Telehealth Flexibilities. Feb 3, 2026.
- Montenegro N. Health Care Extenders: Key Provisions in the Consolidated Appropriations Act, 2026. American Action Forum. Jan 29, 2026.
- Centers for Medicare & Medicaid Services. Telehealth (CY2026 Physician Fee Schedule; Medicare Telehealth Services List).
- Calendar Year 2026 Hospital Outpatient Prospective Payment System (OPPS) and Ambulatory Surgical Center Final Rule (CMS-1834-FC)
- Medicare Program: Hospital Outpatient Prospective Payment and Ambulatory Surgical Center Payment Systems
- ACC, Highlights From the 2026 Hospital OPPS Final Rule
- Telehealth.HHS.gov. Medicare payment policies (telehealth flexibilities through December 31, 2027).
- Thomas RJ, Beatty AL, Beckie TM, et al. Home-Based Cardiac Rehabilitation: A Scientific Statement From the AACVPR, AHA, and ACC. Circulation. 2019;140(1):e69-e89.
- U.S. Congress. H.R.7148, Consolidated Appropriations Act, 2026. 119th Congress.
- Centers for Disease Control and Prevention. Heart Disease Facts.
Disclaimer: This article is for general educational purposes and is not legal, billing, or reimbursement advice. Medicare rules and effective dates can change; providers should verify current CMS guidance and individual payer policies before delivering or billing for services.