ICD-10 Codes for Cardiac Rehab Referral: A 2026 Guide to Qualifying Diagnoses

Few things stall a cardiac rehab referral faster than a diagnosis-code problem. The qualifying conditions are well defined, but the codes that document them, the timing rules, and contractor-specific edits trip up busy practices daily, and the result is a denied claim and a delayed patient. This guide lays out the qualifying conditions and the ICD-10-CM codes commonly used to support them. Treat it as a working reference, not a substitute for your payer's current policy.
How Cardiac Rehab Coverage Actually Works
It helps to separate two things that are easy to conflate. The qualifying condition is what makes a patient eligible for cardiac rehab, and it is set nationally by CMS through National Coverage Determination 20.10 and the regulation at 42 CFR 410.49. The ICD-10-CM code is simply how you document that condition on the claim. Coverage follows the condition, and the code proves it.
This matters because cardiac rehab CPT and HCPCS codes (93797, 93798, G0422, and G0423) are subject to procedure-to-diagnosis editing. If the claim does not carry a diagnosis code on the covered list, the edit denies it automatically as not medically necessary. The covered-code list lives in your MAC's Billing and Coding Article, such as Article A53775, and the record must support whatever you submit.
The Qualifying Conditions for Cardiac Rehab
Under current Medicare rules, the following conditions qualify a patient for cardiac rehabilitation:
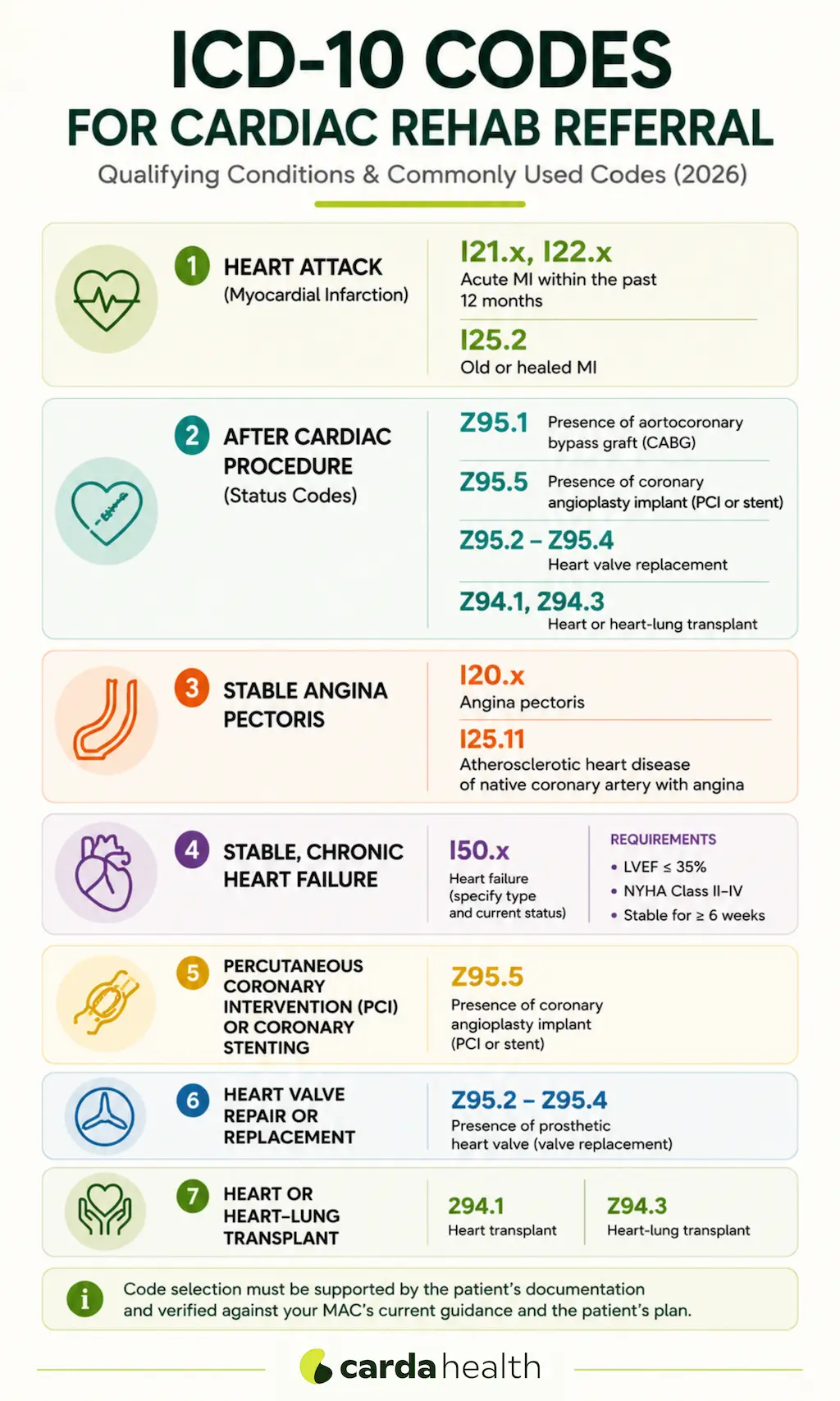
- An acute myocardial infarction within the preceding 12 months
- Coronary artery bypass graft (CABG) surgery
- Current stable angina pectoris
- Heart valve repair or replacement
- Percutaneous coronary intervention (PCI) or coronary stenting
- Heart or heart-lung transplant
- Stable, chronic heart failure (added by NCD 20.10.1), with the specific criteria noted below
The codes below are commonly used to document each of these. They are a starting point, not a guarantee of payment: confirm the exact, current codes in your MAC's Billing and Coding Article and the patient's plan.
ICD-10 Codes by Qualifying Condition
Heart Attack (Myocardial Infarction)
I21.x and I22.x, Acute MI Within the Past 12 Months
The I21 family codes an acute MI by type and site, for example I21.4 for NSTEMI and I21.0 through I21.3 for STEMI by location, while I22.x codes a subsequent MI. These apply when the infarction occurred within the preceding 12 months, the window Medicare allows for the MI-based referral. Document the event date, because timing is part of the coverage rule. For recovery context, see our guide to cardiac rehab after a heart attack.
I25.2, Old or Healed MI
Use I25.2 once the infarction is more than 28 days old. This carries a patient whose qualifying MI has healed but still falls within the 12-month window. A common error is leaving an acute I21 code on the claim long after the event, so switch to I25.2 at the appropriate point and keep the event date documented.
After a Cardiac Procedure (Status Codes)
Referrals after a procedure are usually documented with a status (Z) code that reflects what the patient has had done, rather than an acute diagnosis.
Z95.1, Presence of Aortocoronary Bypass Graft (CABG)
Z95.1 documents that the patient has a coronary artery bypass graft in place and is the code typically used to support a post-CABG cardiac rehab referral.
Z95.5, Presence of Coronary Angioplasty Implant (PCI or Stent)
Z95.5 indicates the presence of a coronary angioplasty implant or graft and supports referrals after PCI or stent placement.
Z95.2 to Z95.4, Heart Valve Replacement
For valve repair or replacement, the code depends on the valve type: Z95.2 for a prosthetic (mechanical) heart valve, Z95.3 for a xenogenic (tissue) valve, and Z95.4 for other heart-valve replacement. Select the one that matches the operative record.
Z94.1 and Z94.3, Heart or Heart-Lung Transplant
Z94.1 documents heart transplant status and Z94.3 documents heart-lung transplant status, supporting cardiac rehab referrals for transplant recipients.
Stable Angina Pectoris
I20.x and I25.11x, Angina Codes
Stable angina is commonly captured with I20.8 or I20.9, or with the atherosclerotic-heart-disease-with-angina codes in the I25.11x family (for example I25.110, I25.118, I25.119). Coverage applies to current, stable angina, so the documentation should reflect that the angina is present and stable rather than resolved.
Stable, Chronic Heart Failure
I50.x, With the LVEF and NYHA Criteria
Heart failure is coded from the I50 family by type, such as I50.22 for chronic systolic heart failure or combined codes like I50.42. The code alone is not enough here: NCD 20.10.1 covers stable, chronic heart failure only when the patient has an LVEF of 35% or less and NYHA class II to IV symptoms despite at least six weeks of optimal therapy, and is stable (no major cardiovascular hospitalization or procedure in the prior six weeks or planned in the next six months). Document the ejection fraction and NYHA class. For clinical context, see our guide to cardiac rehab for heart failure.
Conditions That Do Not Automatically Qualify for Cardiac Rehab
One of the most common referral mistakes is assuming that any cardiovascular diagnosis qualifies a patient for cardiac rehabilitation. Under Medicare's National Coverage Determinations (NCDs), eligibility is based on specific qualifying conditions, not simply the presence of heart disease. If a patient's diagnosis falls outside the covered indications, the referral may be denied unless another qualifying condition is documented.
It's important to remember that these conditions may exist alongside a covered qualifying diagnosis. For example, a patient with atrial fibrillation who recently underwent CABG surgery or experienced an acute myocardial infarction may still qualify for cardiac rehabilitation because of the qualifying event, not because of the atrial fibrillation itself.
When eligibility is uncertain, verify the patient's diagnosis against your Medicare Administrative Contractor's (MAC's) current Billing and Coding Article and review the applicable National Coverage Determination before submitting the referral.
Standard CR vs. Intensive CR (ICR): Does the Diagnosis List Change?
The qualifying conditions for intensive cardiac rehab are largely the same as for standard CR, but ICR is governed by its own rule, NCD 20.31, and is billed with G0422 and G0423 rather than 93797 and 93798. If you refer to an ICR program, confirm the patient's condition is covered under the ICR determination specifically, since indications and updates can differ.
Why Cardiac Rehab Claims Get Denied
Most diagnosis-related denials trace back to a short list of avoidable issues:
- The diagnosis code is not on the MAC's covered list, so the procedure-to-diagnosis edit denies the claim automatically
- A timing rule is missed, such as an MI outside the 12-month window or an acute code used when a status or old-MI code applies
- Documentation does not support medical necessity, for example a heart failure referral without the LVEF and NYHA class recorded
- MAC or payer variation, where a code accepted by one contractor or plan is not accepted by another
Best Practices to Keep the Referrals Clean
To keep referrals clean and compliant, confirm that the patient has a qualifying condition under the relevant National Coverage Determination (NCD). Select the ICD-10-CM code that accurately reflects the patient's condition and current clinical status, and include the event or procedure date whenever timing is a factor in coverage determination.
For patients with heart failure, be sure to document both the left ventricular ejection fraction (LVEF) and New York Heart Association (NYHA) functional class. Before submitting the referral, verify the diagnosis code against your Medicare Administrative Contractor's (MAC's) current Billing and Coding Article as well as the patient's specific health plan requirements.
Finally, ensure that the medical record clearly supports the medical necessity of the services being billed.
For the 2026 reimbursement and telehealth backdrop, see our overview of telehealth cardiac rehab in 2026.
.webp)
The Bottom Line
Clean referrals come down to one principle: match the right ICD-10-CM code to a genuine qualifying condition, document the timing and clinical criteria, and verify against current MAC and payer policy before you submit. Get that right and the referral goes through, the patient starts sooner, and your denial rate drops. Always defer to the current Billing and Coding Article for your contractor, since codes and coverage change.
Frequently Asked Questions
What ICD-10 codes qualify a patient for cardiac rehab?
There is no single code. Coverage follows the qualifying condition, and the code documents it. Commonly used codes include I21.x or I25.2 (heart attack), Z95.1 (CABG), Z95.5 (PCI or stent), Z95.2 to Z95.4 (valve), Z94.1 (transplant), I20.x or I25.11x (stable angina), and I50.x (heart failure, with the LVEF and NYHA criteria). Confirm against your MAC's current covered list.
Why do cardiac rehab claims get denied for diagnosis?
Usually because the diagnosis code is not on the covered list, a timing rule was missed, or the documentation did not support medical necessity. Cardiac rehab codes are subject to procedure-to-diagnosis editing, so a non-covered or missing diagnosis is denied automatically.
What code is used to refer a patient after CABG or a stent?
After CABG, the status code Z95.1 is typically used, and after PCI or stent placement, Z95.5. These reflect the patient's post-procedure status rather than an acute diagnosis.
How recent must a heart attack be to qualify, and which code applies?
The MI must be within the preceding 12 months. An acute MI is coded with the I21 family, and once the infarction is more than 28 days old it is coded as I25.2 (old MI). Keep the event date documented.
Does heart failure qualify a patient for cardiac rehab?
Yes, under NCD 20.10.1, but with specific criteria: a left ventricular ejection fraction of 35% or less and NYHA class II to IV symptoms despite at least six weeks of optimal therapy, in a clinically stable patient. The LVEF and NYHA class should be documented.
Do the qualifying diagnoses differ for intensive cardiac rehab (ICR)?
The conditions are largely similar, but ICR is governed by its own determination (NCD 20.31) and billed with G0422 and G0423 instead of 93797 and 93798. Confirm the patient's condition is covered under the ICR rule specifically.
Where do I find the official, current covered-code list?
In your Medicare Administrative Contractor's Billing and Coding Article (for example A53775) and the relevant NCDs in the CMS Medicare Coverage Database, plus the individual payer's policy for non-Medicare plans.
References
- Centers for Medicare & Medicaid Services. NCD 20.10, Cardiac Rehabilitation Programs.
- Centers for Medicare & Medicaid Services. NCD 20.10.1, Cardiac Rehabilitation Programs for Chronic Heart Failure.
- Centers for Medicare & Medicaid Services. NCD 20.31, Intensive Cardiac Rehabilitation Programs.
- Centers for Medicare & Medicaid Services. Billing and Coding: Frequency and Duration for Cardiac Rehabilitation and Intensive Cardiac Rehabilitation (A53775).
- Code of Federal Regulations. 42 CFR 410.49, Cardiac rehabilitation program and intensive cardiac rehabilitation program.

.avif)

